by Ben Sweetlove | Oct 21, 2025 | QUFW News
Non-invasive prenatal testing (NIPT) has become an important part of early pregnancy care, giving parents insight into their baby’s chromosomes through a simple blood test. But even if NIPT has been done, the 13 week ultrasound is still essential. For parents, it offers a first real look at how the baby is physically developing: seeing the heartbeat, movements, and early features that blood tests alone can’t show. For clinicians, this scan provides anatomical and placental information that NIPT cannot detect, such as structural abnormalities, growth patterns, and chorionicity in multiple pregnancies. Together, NIPT and ultrasound form a more complete picture, combining genetic information with visible evidence of development and maternal health.
In this fact sheet, we will explore:
- What NIPT Does and Doesn’t Do
- Key Assessments at 13 Weeks
- Detecting Early Concerns
- Screening for Maternal Health
- How Results Shape Care
—————
1. What NIPT Does and Doesn’t Do
NIPT is a powerful tool, but it has limits. For parents, it’s helpful to know what questions a blood test can answer — and what still requires an ultrasound. For clinicians, understanding the complementary role of each test ensures a balanced approach to screening.
What NIPT does well:
- Detects common chromosomal conditions such as Trisomy 21 (Down syndrome), Trisomy 18, and Trisomy 13
- Can also check for sex chromosome conditions (depending on the test type)
- Provides a high degree of accuracy, reducing the need for some invasive tests
- Uses a simple blood sample, posing no risk to the pregnancy
What NIPT doesn’t do:
- Does not check the baby’s anatomy or detect structural abnormalities
- Cannot show how the placenta is forming or functioning
- Cannot confirm growth, heartbeat, or the number of babies
- May still require follow-up ultrasound or diagnostic testing if results are high risk
| NIPT |
13 Week Ultrasound |
| Analyses cell-free placental DNA in maternal blood |
Provides a real-time view of the baby and placenta |
| Detects chromosomal abnormalities with high sensitivity and specificity |
Detects structural abnormalities (brain, face, spine, heart, limbs, abdomen and abdominal wall) |
| Non-invasive to the pregnancy, no physical risk to the developing fetus |
Non-invasive, visual reassurance for parents |
| Cannot assess physical growth or maternal health risks |
Screens for preeclampsia risk and placental development |
| Often done from 10 weeks onwards |
Performed between 13 weeks and 13 weeks 6 days |
In practice, NIPT answers questions about chromosomes, while the 13 week ultrasound answers questions about development and health.
2. Key Assessments at 13 Weeks
During the 13 week ultrasound, several important checks are carried out to build a clear picture of how the pregnancy is progressing. The scan confirms the baby’s heartbeat and viability, providing reassurance while also establishing cardiac activity, rhythm, and rate. Growth is measured through the crown–rump length, which is the most accurate way to confirm gestational age and due date between 11 and 14 weeks.
The scan may also determine the number of babies, if not confirmed during an early dating/viability scan, confirming whether it is a single or multiple pregnancy. In multiple pregnancies, chorionicity and amnionicity are identified, which are essential for planning care. Placental development is reviewed, with the location and attachment site documented so any early concerns can be monitored.
Finally, an early anatomy review is performed, allowing a first assessment of the brain, face, heart, spine, abdomen, abdominal wall, limbs, and other structures. While detailed anatomy scans follow later in pregnancy, this early survey can sometimes detect major abnormalities, giving families and clinicians valuable information sooner.
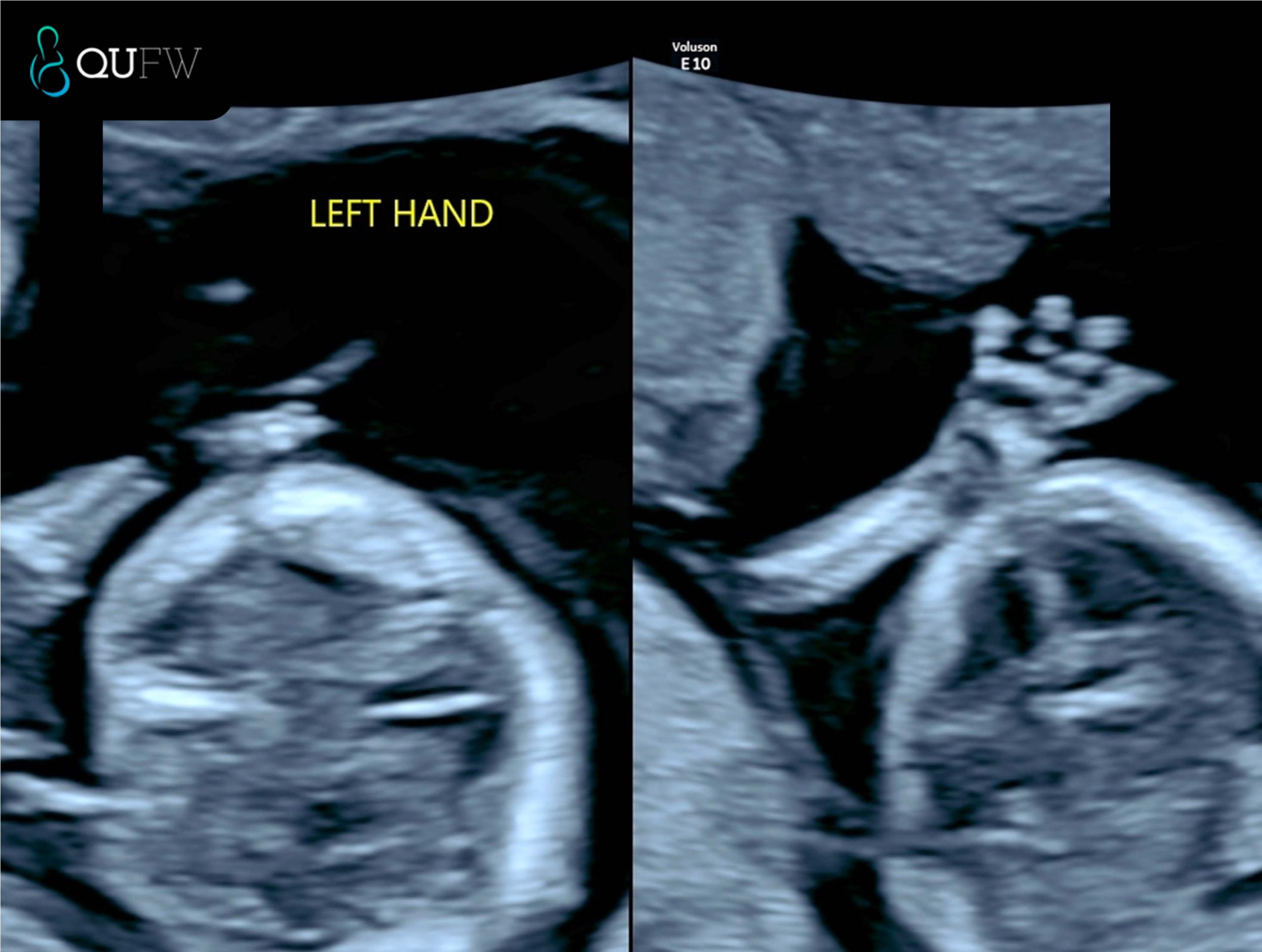
Early structural assessment of the upper limbs
3. Detecting Early Concerns
One of the main strengths of the 13 week ultrasound is its ability to highlight potential issues earlier in pregnancy, giving families more time to understand their options and clinicians more time to plan care.
Areas where concerns may be detected include:
- Structural abnormalities such as issues with the brain, face, spine, abdomen, abdominal wall, or limbs
- Chromosomal indicators like increased nuchal translucency or absent nasal bone
- Placental concerns that could affect growth and development later in pregnancy
- Signs of complications in multiple pregnancies, such as unequal sharing of the placenta
| Possible Concern |
What the Scan May Show |
Next Steps |
| Brain or skull abnormality |
Absence of skull bones (acrania), irregular brain structure |
Referral for detailed scan, genetic counselling |
| Facial structures |
Absence of the Nasal bone, suggestion of early features of cleft lip/palate, facial development of the orbits |
Referral for detailed scan, genetic counselling |
| Spinal abnormality |
Abnormal curvature, incomplete closure of spine |
Specialist ultrasound, ongoing monitoring |
| Abdominal structures |
Presence of stomach, diaphragm, bladder, kidneys, 3 vessel cord |
|
| Abdominal wall defect |
Organs seen outside abdominal cavity as in exomphalos, gastroschisis |
Referral to tertiary care, surgical planning |
| Increased NT or absent nasal bone |
Higher chance of chromosomal condition
Further assessment of fetal cardiac structures |
Follow-up with NIPT, CVS, or amniocentesis
Further cardiac evaluation in the event that the NT measures >3.5mm and low risk NIPT or normal karyotype has been performed. |
| Placental issues |
Abnormal attachment such as early detection of Placenta Accreta Spectrum. |
Monitoring, follow-up scans later in pregnancy |
| Twin complications |
Discordant growth, shared placenta risks |
Closer surveillance, specialist input |
By identifying these concerns early, the 13 week scan helps guide whether further investigations or specialist referrals are needed. It is not a diagnosis on its own but an important first step in recognising when closer attention may be required.
Early structural assessment of the spine
4. Screening for Maternal Health
The 13 week ultrasound also provides information about the mother’s health and how the pregnancy may progress. A key focus at this stage is the risk of preeclampsia, a condition that can cause high blood pressure and complications later in pregnancy. The scan can be combined with maternal blood pressure readings, blood test results, and medical history to estimate the likelihood of developing preeclampsia. If a higher risk is identified, early interventions such as low-dose aspirin and closer monitoring can be recommended, improving outcomes for both mother and baby.
Placental development is another area of assessment. The position and quality of the placenta are reviewed to ensure it is developing normally and providing adequate support for the pregnancy. Identifying placental issues early helps clinicians plan follow-up care and keep a close watch on the baby’s growth throughout the second and third trimesters.
5. How Results Shape Care
The results of the 13 week ultrasound, especially when considered alongside NIPT, shape how care is managed for the rest of the pregnancy. Together, the two tests provide a comprehensive view: NIPT offers insight into the baby’s chromosomes, while ultrasound shows physical development, placental function, and maternal health factors. This combined approach helps guide decisions about further testing, the need for specialist referrals, and the level of monitoring required.
For parents, this means reassurance that the pregnancy is being tracked with the best tools available, and that potential issues can be identified earlier rather than later. For clinicians, it provides a structured baseline that supports personalised care throughout the pregnancy.
The 13 week ultrasound is therefore much more than a milestone moment to see the baby on screen. It is a pivotal point in early pregnancy care, one that combines emotional connection with medical precision. Used together with NIPT, it ensures families and healthcare providers have the clearest possible picture to support a safe and healthy journey ahead.
====================
Content Disclaimer
The information provided on this website is for educational and informational purposes only. It is not intended as a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your obstetric doctor or other qualified provider with any questions you may have regarding a medical condition or treatment and before undertaking a new healthcare regimen.
The content on this website is not intended to be a comprehensive source of information on any particular topic and should not be relied upon as such. The authors and publishers of this website are not liable for any damages or injury resulting from the use or misuse of the information provided on this website.
by Ben Sweetlove | Oct 21, 2025 | QUFW News
The 13 week ultrasound is one of the most important early scans in pregnancy. Usually performed between 13 weeks and 13 weeks 6 days, it gives parents a first detailed look at their baby’s growth and development, often providing reassurance as they see the heartbeat, movements, and forming features. At the same time, this scan holds significant clinical value. It marks the end of the first trimester, when crown–rump length measurement is most accurate for dating the pregnancy, nuchal translucency assessment is most reliable, and an early structural survey can detect major anomalies. These combined insights make the 13 week ultrasound both a meaningful milestone for parents and a cornerstone of first trimester screening and early pregnancy care.
This fact sheet covers these topics:
- Why the 13 Week Scan Matters
- Early Anatomy Check
- Chromosomal Abnormality Screening
- Maternal Health Screening
—————
1. Why the 13 Week Ultrasound Matters
The 13 week ultrasound plays a key role in checking that your pregnancy is progressing as expected. It confirms your baby’s heartbeat, measures growth, and if not confirmed in an earlier viability ultrasound can identify whether you are carrying one baby or multiples. Its major purpose is to assess the early anatomical structures that have developed by 13 weeks. The scan can also assess the placenta to check its position is appropriate at this early gestation, however it is important to note that placental position is largely checked at the 20 week morphology assessment. For parents, these checks bring reassurance that things are on track, while for clinicians, they provide vital data for guiding care for the ongoing pregnancy.
At this stage, crown–rump length measurement helps establish accurate gestational age, chorionicity can be determined in multiple pregnancies, and the position of the placenta is documented. Together, these findings set the foundation for monitoring both maternal and fetal health as the pregnancy continues.
2. Early Anatomy Check
At around 13 weeks, ultrasound technology allows a first look at your baby’s developing anatomy. For parents, this is often the first time you see just how much detail has already formed, including tiny hands and feet, the curve of the spine, and the outline of the brain. For clinicians, this scan provides a systematic review of early structures that can reveal major anomalies at an earlier stage than later pregnancy scans.
Key areas assessed include:
- Brain, skull and face – ensuring the skull is formed, the brain appears normal for this gestational age and the early facial structures are developed
- Spine – checking alignment and early closure of the neural tube
- Heart – confirming rhythm and looking at the early chambers
- Abdomen and abdominal wall – ruling out major structures such as diaphragm, stomach, kidneys, bladder and abdominal wall defects
- Limbs – confirming presence and movement of arms and legs
| What parents see |
What clinicians assess |
| Baby’s profile, head, and movements |
Cranial structure, early detection of acrania or anencephaly, early brain development and evidence of early signs of Open Neural Tube Defects (ONTD’s)
Early facial structures and early detection of facial clefts. |
| Curved spine on screen |
Spinal alignment and signs of neural tube defects |
| Tiny heartbeat flicker |
Cardiac rhythm, chamber development |
| Wriggling arms and legs |
Limb formation, detection of limb reduction anomalies |
| Abdomen outline |
Integrity of the abdominal wall, exclusion of exomphalos or gastroschisis |
| Abdomen |
Abdominal structures such as the diaphragm, stomach filling, presence of both kidneys, appropriate bladder filling, evidence of 3 vessel cord and cord insertion. |
For parents, these images are a reassuring sign of normal growth. For clinicians, they provide a vital opportunity to detect significant problems early, allowing for referral to specialist care if required.
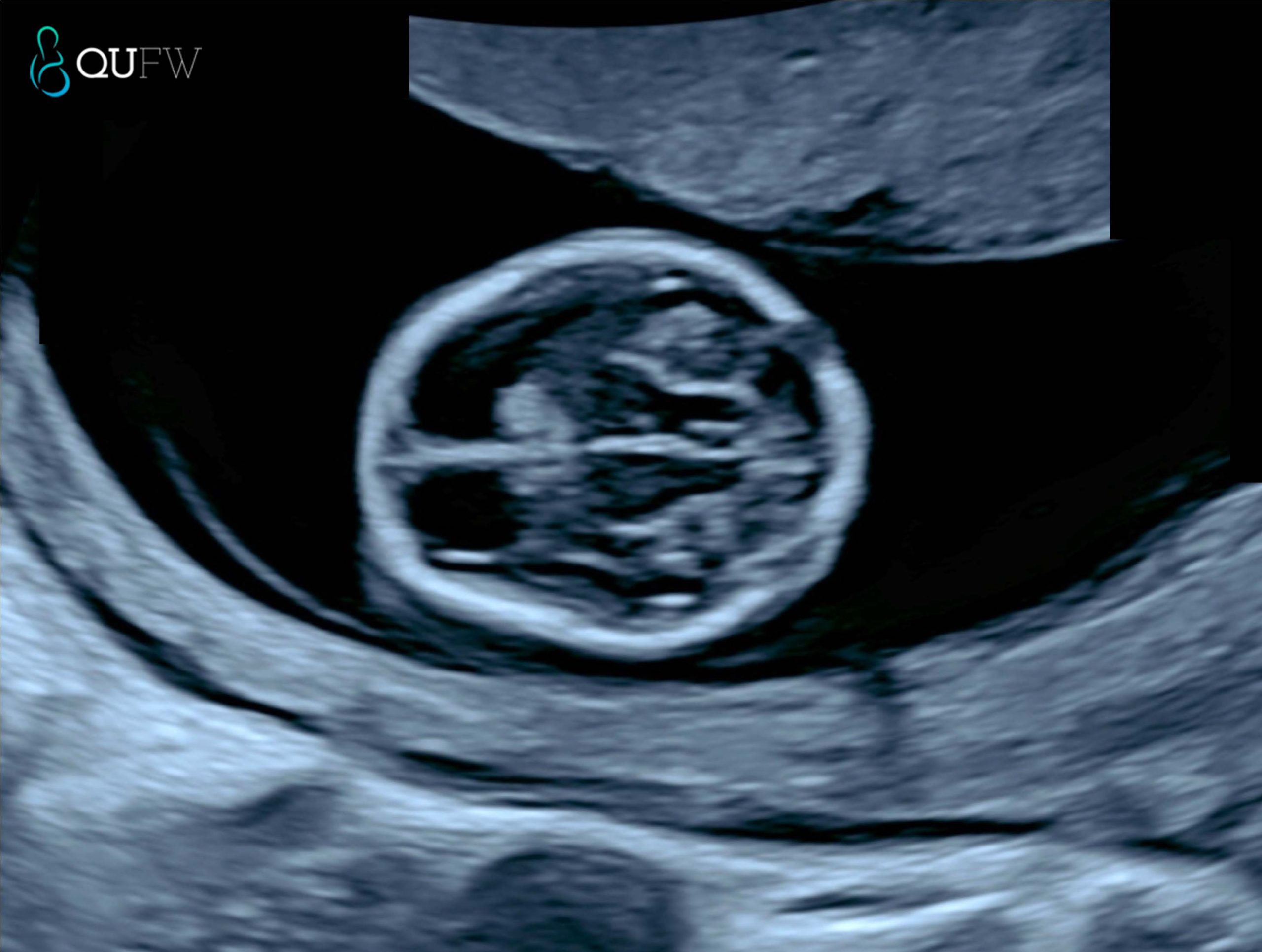
Early structural assessment of the fetal brain
3. First Trimester Combined Screening – Chromosomal Abnormality Screening
The 13 week ultrasound can also help assess the risk of chromosomal conditions, such as Down syndrome (Trisomy 21), Trisomy 18, and Trisomy 13.
In the absence of NIPT screening, a First Trimester Combined Screening (FTCS) may be performed to provide a risk assessment screening for Trisomy 21, Trisomy 18 and Trisomy 13 by utilising the risk assessment algorithm provided by the Fetal Medicine Foundation. An early anatomy assessment scan is performed at the same time as the FTCS assessment.
In the event that a NIPT screening has been performed, it has been recommended by ISUOG International Society of Ultrasound in Obstetrics and Gynaecology under the consensus statement that “First-trimester risk estimates for trisomies 21, 18 and 13 based on nuchal translucency measurements and maternal biochemistry should not be computed in a woman who has already received a normal NIPT result for these trisomies” (reference here).
The Fetal Medicine Foundation (FMF) algorithm is a first-trimester prenatal screening method for Trisomy 21 (Down Syndrome) that uses maternal age, fetal nuchal translucency (NT) ultrasound measurements, and maternal serum markers (free beta-hCG and PAPP-A) to calculate a risk score. The algorithm helps identify pregnancies at higher risk for Trisomy 21, but it’s a screening tool, not a diagnostic test, and a higher risk score may lead to further invasive tests like amniocentesis or chorionic villus sampling (CVS).
How the FMF Algorithm Works
- Maternal Age: Maternal age is a fundamental factor, as the risk of Down Syndrome increases with maternal age.
- Ultrasound (NT Measurement): A detailed first-trimester ultrasound is performed to measure the nuchal translucency (NT), a collection of fluid at the back of the fetus’s neck.
- Biochemical Markers: Maternal blood is tested for two hormones:
- Free beta-hCG (free beta-human chorionic gonadotropin): Typically elevated in Down Syndrome pregnancies.
- PAPP-A (pregnancy-associated plasma protein-A): Generally lower in Down Syndrome pregnancies.
- Risk Calculation: The FMF algorithm combines these factors to generate a personalised risk for Trisomy 21, Trisomy 18 and Trisomy 13.
For parents, this part of the scan offers important reassurance or an early signal that further testing may be needed. For clinicians, it provides measurable markers that contribute to first-trimester combined screening.
Markers typically assessed at this stage include:
- Nuchal translucency (NT): a fluid space at the back of the baby’s neck that, if increased, can indicate a higher chance of chromosomal abnormality.
- Nasal bone: its presence or absence can be a significant marker in risk assessment.
- Ductus venosus flow: abnormal flow patterns may be associated with aneuploidy or cardiac defects.
- Tricuspid regurgitation: when present, it can increase the risk profile.
| For parents |
For clinicians |
| The scan looks at small features, like the fluid behind the baby’s neck and nose bone, that can indicate a higher or lower chance of conditions such as Down syndrome. |
NT is measured between 11+0 and 13+6 weeks when CRL is 45–84 mm; when combined with maternal serum biochemistry (free β-hCG, PAPP-A), this forms the basis of first-trimester combined screening.
It is preferred at QUFW to perform this assessment between 13 weeks and 13+6 days |
| A higher-than-expected NT doesn’t mean something is wrong, but it may lead to follow-up testing for clarity particularly for congenital heart defects or other genetic syndromes. |
Integration of ultrasound markers with serum and maternal age yields detection rates of >90% for Trisomy 21 at a 5% false-positive rate.
In the event of an NT measurement >3.5mm, further structural assessment of the fetus including the heart for congenital heart defects is made as part of the early anatomy scan. |
| Results can help guide whether additional tests, such as NIPT or diagnostic procedures (CVS, amniocentesis), are recommended. |
Ancillary markers (nasal bone, ductus venosus, tricuspid regurgitation) improve specificity and refine risk stratification. |
In practice, this means the 13 week scan is more than just a “look at the baby” moment. It forms a crucial part of early screening that combines visual markers, blood tests, and clinical context to give the clearest picture possible at this stage of pregnancy.
Nuchal translucency assessment
4. Maternal Health Screening
The 13 week ultrasound is not only about checking the baby, it also provides valuable information about the mother’s health. For parents, this means doctors can look for early signs of conditions that could affect the pregnancy, helping to keep both mother and baby safe. For clinicians, this scan offers an opportunity to assess maternal risk factors and build a plan for ongoing care.
One of the key conditions that can be screened for is preeclampsia, a complication that can lead to high blood pressure and other serious health issues later in pregnancy. At this stage, the scan can be combined with blood pressure readings, maternal history, and blood test results to estimate a woman’s risk. If the risk is found to be higher, preventive steps can be started early.
The scan may also highlight placental concerns. Early assessment of how the placenta is developing and where it is attached provides important insight into how well it might support the pregnancy. These checks give reassurance to parents while helping clinicians take proactive measures if any issues are identified
====================
Content Disclaimer
The information provided on this website is for educational and informational purposes only. It is not intended as a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your obstetric doctor or other qualified provider with any questions you may have regarding a medical condition or treatment and before undertaking a new healthcare regimen.
The content on this website is not intended to be a comprehensive source of information on any particular topic and should not be relied upon as such. The authors and publishers of this website are not liable for any damages or injury resulting from the use or misuse of the information provided on this website.
by Ben Sweetlove | Oct 21, 2025 | QUFW News
In early pregnancy, you might hear a range of terms used for the scans you might need, such as “viability,” “dating,” “early anatomy,” or “NIPT.” These names can sound similar, and it’s not always clear how they differ or when each one is recommended.
This fact sheet explains the different types of early pregnancy scans so you can understand their purpose and timing. It answers the following questions:
- Overview of first-trimester scans
- Dating and Viability scan (around 6–12 weeks)
- Early Anatomy scan (13–13+6 weeks)
- First Trimester Combined Screening (FTCS) (13–13+6 weeks)
- NIPT and its timing
- Which scan should I book first?
—————
1. Overview of first-trimester scans
In the first trimester, ultrasound can confirm pregnancy, check wellbeing, and estimate due dates.
Common scans include:
- Viability and Dating scan – a viability scan or a dating scan refer to the same thing and involve an early check of pregnancy location and heartbeat. The Sonographer measures the fetus to establish or confirm an estimated due date (EDD)
- Early Anatomy scan – assesses early anatomy and screens for certain structural conditions
- First Trimester Combined Screening scan – this scan is the same as the Early anatomy scan but provides additional screening for chromosomal abnormalities, particularly Trisomy 21, 18 and 13. The risk assessment is only performed if the patient has not had a NIPT performed. The NIPT has a higher detection rate for Trisomy 21 (almost 99% detection rate) as opposed to approximately 90% detection rate.
- NIPT (non-invasive prenatal testing) – blood test for chromosomal screening, recommended to be accompanied alongside a viability ultrasound.
Here’s a breakdown of each of these scans:
2. Dating and Viability scan (around 6–12 weeks)
A viability scan confirms that the pregnancy is in the uterus, checks for a heartbeat, and assesses early development. A dating scan measures the crown–rump length (CRL) to estimate gestational age and your EDD. This timing offers a high degree of accuracy (± 5 days). You may be referred for a viability scan if you:
- Have pain or bleeding
- Have had an ectopic pregnancy before
- Conceived via IVF
- Have a history of pregnancy loss
It also confirms:
- The baby’s heartbeat
- Whether you are carrying one baby or multiples
- The pregnancy location
If performed very early (before 6 weeks), it may be too soon to see a heartbeat, and a repeat scan may be needed.
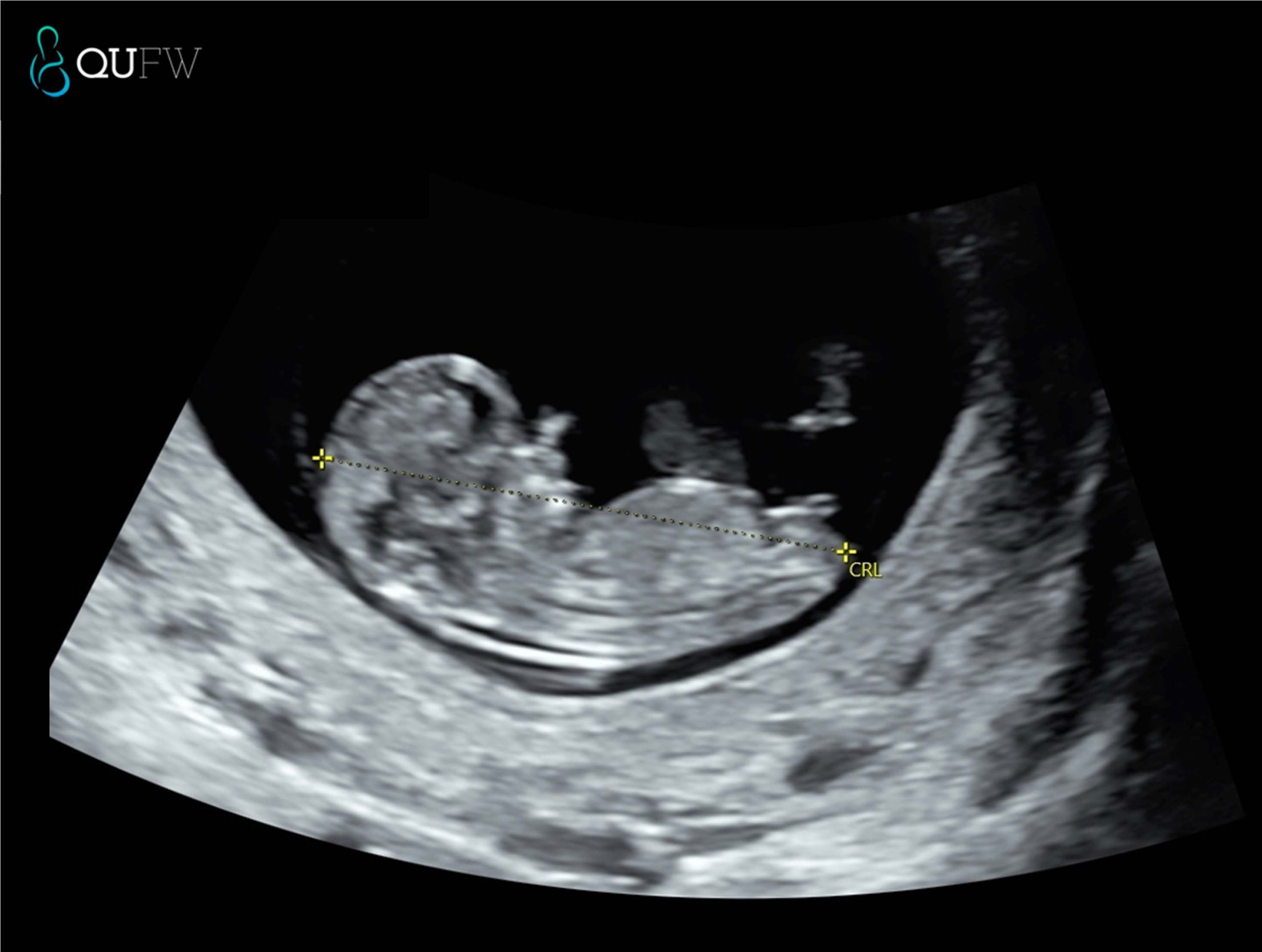
Dating scan prior to NIPT
3. Early Anatomy scan (13–13+6 weeks)
The Early Anatomy scan assesses early development and screens for specific structural anomalies. At QUFW we also perform a risk assessment for pre-eclampsia at this scan. The early anatomy scan is performed in conjunction with an NIPT. If you elect not to have NIPT then you will be asked if you would like a risk assessment for Trisomy 21, 18 and 13 (the most common chromosomal anomalies) performed in addition to the anatomical assessment, in which case this then becomes a FTCS (see below).
It also checks:
- Heartbeat
- Cervical length assessment
- Placenta position
- Multiple pregnancy details
4. If the scan’s EDD differs from your LMP-based date, your healthcare provider will usually use the ultrasound date.
This is the same as an early anatomy scan, however we provide a risk assessment for chromosomal abnormalities like Trisomy 21, 18, and 13. As a screening for Down Syndrome, it has approx. 90% detection rate when combining the following factors such as
- Maternal age and background risk
- Ultrasound markers such as nuchal translucency, nasal bone, fetal heart rate
- Maternal serum biochemistry (Free beta-hCG and PAPP-A)
At QUFW, similar to the Early Anatomy scan we also perform a pre-eclampsia risk assessment as part of this scan.
Nuchal translucency assessment
5. NIPT and its timing
NIPT is a blood test that can be done from around 10 weeks of pregnancy. At QUFW, we prefer to book NIPT’s from 10 weeks 2 days at the earliest.
It analyses small fragments of the baby’s DNA in the mother’s blood to assess the likelihood of certain chromosomal conditions. NIPT does not replace ultrasound which assesses for structural abnormalities.
6. Which scan should I book first?
It depends on your history and how certain you are of your dates:
- Uncertain LMP or irregular cycles – dating and viability scan between 7–12 weeks
- History of pregnancy complications – Viability and dating scan from 6 weeks gestation
- IVF conception – viability scan at 6–7 weeks, then Early Anatomy scan at 13–13+6 weeks
- Known LMP and no risk factors – dating and viability scan between 7-12 weeks, followed by an Early Anatomy scan. Your GP or specialist will recommend a plan suited to your circumstances.
FAQs
Is a viability scan the same as a dating scan?
A viability and dating scan is essentially the same scan and confirms the presence of a pregnancy in the correct location, if it is a multiple pregnancy and confirms that a heart beat is present. It is also used to either confirm or establish correct dating or due date for the pregnancy.
Do I need both Early Anatomy and NIPT?
A NIPT is a screening test for chromosomal abnormalities. It does not detect structural or developmental concerns with the developing fetus. It is advised that an Early Anatomy scan is performed between 13 – 13 weeks 6 days as a structural assessment of your baby. At QUFW we also perform a Preeclampsia screening as a component of the Early Anatomy scan. A low probability result for a NIPT, does not exclude a structural concern in a pregnancy.
When is the best time for a dating scan?
Between 7 and 12 weeks for best accuracy.
Can an Early Anatomy scan detect all conditions?
No. It screens for certain conditions but not all genetic or structural differences may be detected at this early gestation. A further morphology scan is recommended between 20-22 weeks to reassess the baby.
====================
Content Disclaimer
The information provided on this website is for educational and informational purposes only. It is not intended as a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your obstetric doctor or other qualified provider with any questions you may have regarding a medical condition or treatment and before undertaking a new healthcare regimen.
The content on this website is not intended to be a comprehensive source of information on any particular topic and should not be relied upon as such. The authors and publishers of this website are not liable for any damages or injury resulting from the use or misuse of the information provided on this website.
by Ben Sweetlove | Oct 21, 2025 | QUFW News
What is a dating scan?
A dating scan is an early pregnancy ultrasound used to measure the developing baby and estimate gestational age. It also confirms the baby’s heartbeat, checks for multiple pregnancies, and verifies the pregnancy location in the uterus.
At QUFW, dating scans are performed by our caring, experienced sonographers using high-resolution equipment to ensure accurate measurement and clear images.
This fact sheet answers the following questions:
- When should I have a dating scan?
- What happens during a dating scan?
- How accurate is a dating scan?
- Do I need a dating scan?
- What is the difference between a dating scan and the 13 week early anatomy scan?
—————
1. When should I have a dating scan?
The most accurate time for a dating scan is between 7 and 10 weeks of pregnancy.
- Before 7 weeks: The scan can confirm a gestational sac and yolk sac from 5 weeks, a heartbeat after 6 weeks, but measurements may be less reliable to confirm viability and dating A gestational sac visualised within the uterus confirms correct pregnancy location.
- Between 7 and 10 weeks: The crown–rump length (CRL) measurement is most accurate for establishing your estimated due date (EDD).
- After 10 weeks: Dating is possible, but accuracy decreases as babies start to vary more in size.
Some people have an earlier scan (6–7 weeks) if they have irregular cycles, are unsure of their last menstrual period (LMP), have conceived through IVF, or have a history of pregnancy complications.
8 week fetus with heartbeat
2. What happens during a dating scan?
At QUFW, your sonographer will:
- Review your referral and confirm your details.
- Explain the scan process and answer any questions.
- Perform the scan using either a transabdominal (across the abdomen) or transvaginal (internal) approach, depending on gestational age and image clarity.
- Measure the CRL, check for heartbeat, number of babies, and other factors such as ovaries. Provide images and send a detailed report to your referring doctor.
Most dating scans take around 15–30 minutes. They are safe, non-invasive, and use no radiation, however we always practice ALARA (As Low As Reasonably Achievable) principles.
3. How accurate is a dating scan?
A dating scan in the first trimester is a reliable way to determine gestational age.
- CRL measurements taken between 7 and 10 weeks are accurate to within ± 5 days.
- Later scans may be less accurate because individual growth patterns vary.
If the scan’s EDD differs from your LMP-based date, your healthcare provider will usually use the ultrasound date.
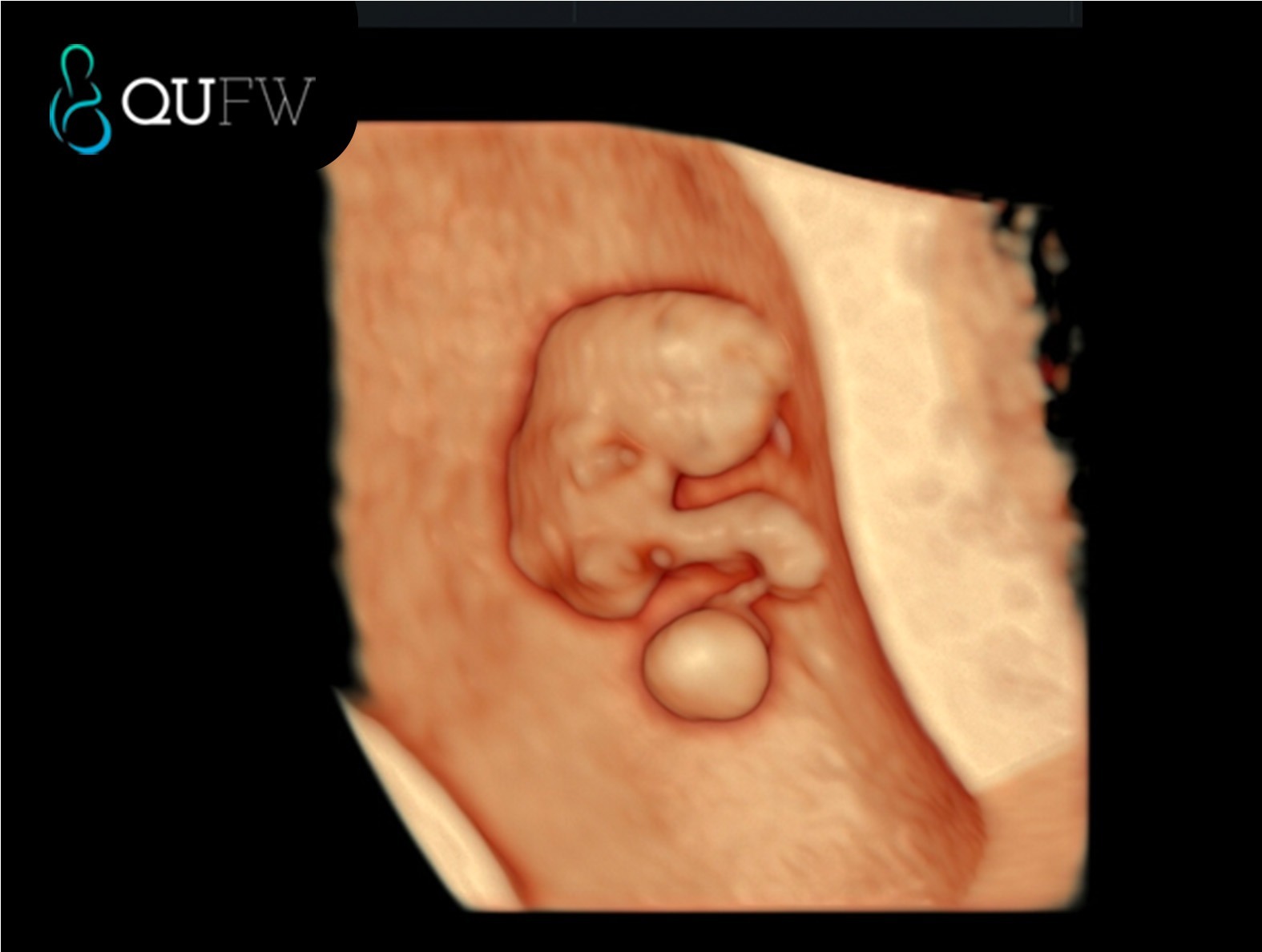
3D image of an 8 week fetus
4. Do I need a dating scan?
You may be advised to have one if:
- You are unsure of your LMP or have irregular cycles.
- You have conceived via assisted reproduction.
- You have a history of early pregnancy loss or ectopic pregnancy.
- Your doctor recommends one for clinical reasons.
5. What is the difference between a dating scan and the 13 week early anatomy scan?
While both are first-trimester ultrasounds, their purposes differ:
| Dating scan |
Early anatomy scan/First Trimester Combined Screening ultrasound |
| 7–12 weeks |
13-13+6 weeks |
| Measures CRL to determine EDD |
Measures CRL to confirm EDD and appropriate growth of baby.
Can be used as a dating scan if no prior dating ultrasound has been performed. |
| Confirms heartbeat, multiples, location of pregnancy |
- Checks early anatomy structures including a heart beat
- In the instance of no prior NIPT, it can provide a First trimester risk assessment for chromosomal abnormalities such as Trisomy 21, 18 and 13 when combined with First trimester blood tests and measuring the fluid at the back of the baby’s neck (Nuchal Translucency)
- Can also provide Pre-eclampsia screening
|
FAQs
Is a dating scan safe?
Yes. Ultrasound is considered safe in pregnancy and does not use radiation.
Can my due date change after a dating scan?
Yes. If ultrasound findings differ from LMP-based dates, your healthcare provider may adjust your due date.
Can a dating scan detect twins?
Yes. A dating scan can confirm if you are carrying more than one baby and whether they share the same placenta or have separate placentas which is important for managing your pregnancy moving forward.
Do I need a full bladder for a dating scan?
For an early dating scan, a partially full bladder may help improve image clarity. Your clinic will confirm preparation instructions when booking.
What if the scan doesn’t show a heartbeat?
If it’s too early in pregnancy, the heartbeat may not be visible yet. Your doctor may recommend repeating the scan in one to two weeks.
Can a dating scan show the baby’s gender?
No. It is too early in pregnancy for accurate gender determination.
====================
Content Disclaimer
The information provided on this website is for educational and informational purposes only. It is not intended as a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your obstetric doctor or other qualified provider with any questions you may have regarding a medical condition or treatment and before undertaking a new healthcare regimen.
The content on this website is not intended to be a comprehensive source of information on any particular topic and should not be relied upon as such. The authors and publishers of this website are not liable for any damages or injury resulting from the use or misuse of the information provided on this website.