QUFW is currently unable to upload ultrasound reports to My Health Record due to a temporary system limitation. In the meantime, all patients will continue to receive a copy of their ultrasound report following their examination, and a copy will also be provided to their referring practitioner. If you would like your ultrasound report to be uploaded to My Health Record once this functionality becomes available, please email [email protected] with your request. We appreciate your patience and understanding and apologise for any inconvenience. — QUFW Management
Having preeclampsia in a previous pregnancy changes how you approach the next one. It is natural to feel a mix of hope and apprehension when you see a positive test, or even when you are still at the planning stage. What happened before stays with you, and it is completely reasonable to want answers before you find yourself back in unfamiliar territory.
The good news is that a previous diagnosis is not a verdict. It is information, and in pregnancy care, information is one of the most useful things you can have.
This fact sheet is for women who have been through preeclampsia before and explains what a subsequent pregnancy might look like. It covers the conversations to have before you conceive, through to the monitoring and management involved.
What is my actual risk of pre-eclampsia happening again?
Recurrence is possible, but it is not inevitable. Research consistently shows that the majority of women who experienced preeclampsia in a previous pregnancy do not develop it again. That said, a prior history remains one of the strongest individual risk factors, and your risk is meaningfully higher than that of someone with no history of the condition.
How high that risk is depends on several factors, including how severe your previous preeclampsia was, how early in the pregnancy it developed, whether it was early-onset (before 34 weeks) or late-onset, and whether any underlying health conditions contributed. Women who had severe or early-onset preeclampsia generally carry a higher recurrence risk than those who developed a milder form later in pregnancy.
This variation is exactly why individual risk assessment matters more than population averages. Your situation is specific to you, and understanding your personal risk profile is the foundation of good planning.
Before you conceive: conversations worth having
One of the most valuable things you can do is speak with your GP or obstetrician before you start trying to conceive. This is not always top of mind, but it can make a real difference to how your next pregnancy is managed.
The Royal Australian and New Zealand College of Obstetricians and Gynaecologists (RANZCOG) recommends that women with a history of preeclampsia be reviewed prior to a subsequent pregnancy to identify and address modifiable risk factors. This pre-conception conversation is a chance to revisit what happened in your previous pregnancy, identify any underlying conditions that may have contributed (such as hypertension, kidney disease, diabetes, or autoimmune conditions), and explore whether anything can be optimised before you fall pregnant again.
For some women, this means getting a chronic condition better controlled. For others, it may simply mean having an early referral pathway in place so that care begins promptly from the moment a pregnancy is confirmed. Either way, starting that conversation early puts you in a stronger position.
How does risk screening differ in my next pregnancy?
The first trimester combined screening for preeclampsia, typically performed at your 13 to 14 week scan, still applies in a subsequent pregnancy and remains a valuable tool. What changes is the weight your history carries within that screening.
A prior history of preeclampsia is factored into the risk calculation alongside your blood pressure readings, blood test markers (including PAPP-A and PlGF), and uterine artery Doppler measurements. Because your previous experience is already a significant risk factor, you may be more likely to receive a high-risk result than someone without that history. This is not the screening working against you. It is the screening working as intended, by accounting for your full picture rather than treating you as a first-time case.
Ultrasound of the blood flow through a uterine artery (Transabdominal assessment of the uterine artery Doppler waveform in the first trimester)
It is also worth understanding that a high-risk result is not a diagnosis. Many women who screen as high-risk go on to have healthy pregnancies without developing preeclampsia. The purpose of early screening is to personalise your care and enable timely intervention where it is needed.
For more detail on what the screening involves and what a high-risk result means, see our article.
Is Aspirin suitable for preeclampsia?
If you have a prior history of preeclampsia, low-dose aspirin will very likely be recommended as a preventative measure in your next pregnancy. For women who have been through peeclampsia before, the reasoning behind this recommendation often lands differently. You already know what it is trying to prevent.
RANZCOG and the Society of Obstetric Medicine of Australia and New Zealand (SOMANZ) both support the use of low-dose aspirin for women at increased risk of preeclampsia. The recommended dose is 150mg taken at night, commenced between 11–14 weeks of pregnancy and continued until 34 to 36 weeks gestation.
Evidence from the ASPRE trial shows that starting aspirin at this dose and timing can reduce the risk of preterm preeclampsia (before 37 weeks) by approximately 62%, and early preeclampsia (before 34 weeks) by approximately 82%. It will not eliminate risk entirely, but it is one of the most effective tools currently available.
Aspirin is considered safe in pregnancy for most women, but always confirm with your treating doctor before commencing, particularly if your circumstances have changed since your last pregnancy, or if you have any known allergies or medical contraindications.
What does a preeclampsia monitoring plan might look like?
Women with a prior history of preeclampsia are typically managed as higher-risk from the outset of a new pregnancy. In practical terms, this means your care will likely include more touchpoints than a standard low-risk pregnancy.
You can expect some or all of the following, depending on your individual circumstances and your treating team’s recommendations: earlier referral to an obstetrician or maternal-fetal medicine specialist, regular blood pressure monitoring throughout the pregnancy, urine testing for protein at antenatal appointments, blood tests to monitor kidney and liver function, additional growth scans in the second and third trimester to assess your baby’s development, and placental function assessment, including Doppler studies, particularly if growth concerns arise.
This level of monitoring can feel intensive, and it is worth acknowledging that more appointments and more testing can themselves become a source of stress. It helps to reframe closer monitoring not as a sign that something is already wrong, but as a deliberate strategy to catch any changes early, when options are broader and outcomes are generally better.
What happens if I get preeclampsia again?
For some women, preeclampsia will develop again despite best efforts at prevention and monitoring. If that happens, earlier detection usually means more options and a more managed response.
Having been through it before, you are also better equipped than most. You are more likely to recognise early symptoms, more likely to know when to escalate a concern, and more likely to have a care team who is already prepared and monitoring closely. None of that eliminates the difficulty, but it does change the experience in meaningful ways.
SOMANZ guidance emphasises that women with recurrent preeclampsia benefit from specialist involvement early in pregnancy, and that a clearly documented management plan, established before symptoms develop, leads to better outcomes for both mother and baby.
Book your 13-week scan at QUFW
At QUFW, preeclampsia risk screening is included as part of our routine 13 to 14 week scan. If you have a history of preeclampsia, this appointment is an important early step in understanding your risk in this pregnancy.
Our team will take into account your full history as part of the screening process. We screen all women at this stage, and we are experienced in supporting those who have been through preeclampsia before.
The information provided on this website is for educational and informational purposes only. It is not intended as a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your obstetric doctor or other qualified provider with any questions you may have regarding a medical condition or treatment and before undertaking a new healthcare regimen.
The content on this website is not intended to be a comprehensive source of information on any particular topic and should not be relied upon as such. The authors and publishers of this website are not liable for any damages or injury resulting from the use or misuse of the information provided on this website.
Fertility investigations can feel overwhelming, particularly when a test is new or unfamiliar. HyFoSy is a straightforward ultrasound procedure, and it’s common for patients to have questions about comfort, what will happen on the day, and how the results may guide next steps in care.
This fact sheet explains what a HyFoSy examination is, why it is performed, and what you can expect before, during, and after your appointment. In this article, Jacqui, Lead Gynaecological Sonographer at QUFW, talks you through the HyFoSy procedure and how it fits into a fertility assessment.
Medical disclaimer: The information provided here is general in nature and intended for educational purposes only. It does not replace medical advice, diagnosis, or treatment. Please speak with your GP or specialist for personalised guidance.
HyFoSy (Hysterosalpingo-Foam Sonography) is a specialised gynaecology ultrasound used as part of a fertility assessment. It evaluates the internal cavity of the uterus and the openness of the fallopian tubes.
“HyFoSy is a specialised gynaecology ultrasound procedure used as part of a fertility assessment,” Jacqui explains in the above video.
The procedure uses a contrast agent called ExEm foam, which is made from a gel and purified water. When mixed, it forms a foam that can be seen clearly on ultrasound.
“It’s used to detect any blockages in the fallopian tubes.”
Unlike X-ray–based tests, HyFoSy is performed entirely under ultrasound guidance and does not involve radiation.
Why does fallopian tube patency matter?
The fallopian tubes play a central role in natural conception.
“The fallopian tubes are an essential part of a woman’s reproductive system, connecting the ovaries to the uterus,” says Jacqui.
For pregnancy to occur:
The ovary must release an egg
The egg must travel through an open fallopian tube
Sperm must meet the egg within the tube
“If both tubes are blocked, the sperm and egg cannot meet, making conception impossible.”
Because fallopian tubes cannot be visualised on a standard pelvic ultrasound, a HyFoSy is used to assess whether they are open (patent).
When is a HyFoSy performed?
Timing is important for safety and accuracy.
“The procedure should be performed between four to ten days after the first day of your last menstrual period,” Jacqui explains.
This timing:
Reduces the chance of early pregnancy
Provides optimal visualisation
Our doctors perform the procedure after a thorough transvaginal assessment of the pelvic organs has been performed by our sonographers.
Patients are advised to contact QUFW on day one of their period to arrange an appointment. If cycles are irregular or infrequent, individual advice is provided.
How do I prepare for a HyFoSy?
Preparation is straightforward and designed to support comfort.
“You do not need a full bladder for the examination,” Jacqui notes.
You may be advised to:
Avoid sexual intercourse before the procedure
Have a pregnancy blood test if required
Take your usual pain relief one hour before the appointment
You are welcome to bring a support person if that feels helpful.
What happens during a HyFoSy?
On arrival, you will complete a urine pregnancy test to confirm you are not pregnant.
A transvaginal ultrasound is performed first to assess the uterus and ovaries. Once this is complete, the doctor will:
Insert a speculum
Place a thin, flexible catheter through the cervix into the uterus
“As the catheter passes through, you may feel some discomfort or cramping,” Jacqui explains.
A small balloon at the end of the catheter is inflated to keep it in place, which may cause brief pressure.
The speculum is then removed, and the transvaginal probe is reinserted. Saline is passed through the catheter to assess the uterine cavity for scarring, fibroids, or polyps.
Then, the ExEm foam is introduced.
“The goal is to see the contrast flow through open tubes and spill into the area surrounding the ovaries.”
Once complete, the catheter and probe are removed.
What will I feel during a HyFoSy?
Experiences vary between patients.
“Some patients may feel light-headed, hot, or dizzy during the procedure,” says Jacqui.
Common sensations include:
Mild to moderate cramping
Period-like discomfort
Temporary pressure
“These symptoms usually settle quickly,” Jacqui reassures.
Patients are encouraged to communicate during the procedure so comfort can be supported.
How long does a HyFoSy appointment take?
“We allow 45 to 60 minutes for the appointment,” Jacqui explains.
The actual HyFoSy procedure typically takes around 10 minutes, with the remainder of the time used for preparation, explanation, and ultrasound assessment.
When and how do I receive HyFoSy results?
As the procedure is performed, findings are usually discussed in real time.
“The doctor will explain the findings and whether the tubes appear open.”
Occasionally, results may be inconclusive due to temporary tubal spasm rather than true blockage.
Your results are:
Sent to your referring doctor
Shared with you via a secure Tricefy link on your mobile
Report timing depends on examination complexity and additional findings.
Is HyFoSy safe and accurate?
HyFoSy is considered a safe and well-tolerated procedure. It does not involve ionising radiation or general anaesthetic.
Studies have shown HyFoSy to have high diagnostic accuracy for tubal patency, comparable to traditional hysterosalpingography (HSG), with better patient comfort and fewer risks.
After the procedure: recovery and care
After a HyFoSy, it is normal to experience:
Watery discharge
Light bleeding or spotting
Mild cramping or bloating
“This is normal and due to the saline and contrast used,” Jacqui explains.
A sanitary pad is provided, and symptoms usually resolve within a day or two. Normal activities, including intercourse, can be resumed.
If you experience:
Severe pelvic pain
Fever
Green or yellow vaginal discharge
you should contact your GP or referring doctor, as these may indicate infection, which is uncommon.
Book your gynaecology scan at QUFW
Fertility investigations can bring up many emotions, including hope, worry, and uncertainty. Having clear information can make the process feel more manageable.
At QUFW, gynaecology scans are performed in a supportive environment using evidence-based techniques and clear communication. Your HyFoSy examination is designed to provide meaningful information to guide your fertility care, while prioritising safety and comfort.
You are supported every step of the way.
References
Exacoustos, C., Di Giovanni, A., Szabolcs, B. et al. (2015). Automated sonographic tubal patency evaluation using contrast agent (HyFoSy). Ultrasound in Obstetrics & Gynaecology, 46(5), 620–627. https://pubmed.ncbi.nlm.nih.gov/19852043/
Dreyer, K., Out, R., Hompes, P. G. et al. (2017). Oil-based or water-based contrast for hysterosalpingography in infertile women. New England Journal of Medicine, 376, 2043–2052. https://www.nejm.org/doi/full/10.1056/NEJMoa1612337
Video transcript
Hi, my name’s Jacqui. I’m the lead gynaecological sonographer for QUFW. I’m here to talk you through your HyFoSy examination at QUFW.
HyFoSy is a specialised gynaecology ultrasound procedure used as part of a fertility assessment. It provides information about the internal cavity of the uterus and the fallopian tubes. A contrast agent, ExEm foam, is used to visualise the tubes. It is made from a gel and purified water which, when mixed, create a foam used to detect any blockages in the fallopian tubes.
Why are patent fallopian tubes important?
The fallopian tubes are an essential part of a woman’s reproductive system, connecting the ovaries to the uterus. Open (or patent) fallopian tubes are important for conception. If both tubes are blocked, the sperm and egg cannot meet, making conception impossible. The fallopian tubes cannot be visualised on a standard ultrasound, which is why the HyFoSy procedure is used.
When the procedure is performed
The procedure should be performed between four to ten days after the first day of your last menstrual period. We recommend calling our office on day one of your period to make a booking. If you have irregular or infrequent cycles, please call for individual advice.
Some patients may be asked to avoid sexual intercourse before the procedure and/or have a pregnancy blood test. You do not need a full bladder for the examination. It’s recommended that you take your usual pain relief about one hour before your appointment. You may bring a support person if you wish, although this is not required.
What happens on the day
On arrival, you’ll be asked to perform a urine pregnancy test to confirm you are not pregnant. A transvaginal ultrasound is done first. Once this is complete, the doctor will insert a speculum and place a thin, flexible catheter through your cervix into the uterus. As the catheter passes through, you may feel some discomfort or cramping. Once it’s in position, a small balloon at the end of the catheter is inflated, which may cause mild pressure that should ease quickly.
The speculum is then removed and the transvaginal probe reinserted so we can visualise the procedure. Saline (a sterile saltwater solution) is passed through the catheter to check the uterine cavity for scarring, polyps, or fibroids that may not be visible on regular ultrasound. Then, the contrast agent (ExEm foam) is passed through the catheter. The doctor observes the contrast as it moves through the uterine cavity and fallopian tubes. The goal is to see the contrast flow through open tubes and spill into the area surrounding the ovaries.
When the procedure is finished, the catheter and probe are removed.
What to expect during a HyFoSy
Some patients may feel light-headed, hot, or dizzy during the procedure. Mild cramping, similar to period pain, is also common. These symptoms usually settle quickly, and pain relief can help if needed. Please tell your doctor or sonographer if you feel unwell, and they’ll help you feel more comfortable.
How long it takes
We allow 45 to 60 minutes for the appointment, including preparation and scanning time. The actual procedure usually takes about 10 minutes.
When you’ll receive your results
As the procedure is performed, the doctor will explain the findings and whether the tubes appear open. Occasionally, results may be inconclusive if it’s difficult to distinguish between tubal spasm and blockage.
Your results will be sent directly to your referring doctor, and you’ll also receive a copy via a secure link through Tricefy on your mobile. The time taken for your doctor to receive the written report will depend on the complexity of the examination and whether additional findings were noted.
After the procedure
You may notice some watery or light bloody discharge afterward. This is normal and due to the saline and contrast used. A sanitary pad will be provided. Mild bloating, cramping, or lower abdominal discomfort can occur and is usually relieved with standard pain medication. Light bleeding or spotting may continue for a day or two.
If you experience severe pelvic pain, fever, or an unusual vaginal discharge that is green or yellow, contact your GP or referring doctor promptly, as these may be signs of infection (which is uncommon).
It is safe to resume normal activities, including intercourse, after the procedure. The HyFoSy is a very safe procedure that does not involve ionising radiation or general anaesthetic.
The information provided on this website is for educational and informational purposes only. It is not intended as a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your obstetric doctor or other qualified provider with any questions you may have regarding a medical condition or treatment and before undertaking a new healthcare regimen.
The content on this website is not intended to be a comprehensive source of information on any particular topic and should not be relied upon as such. The authors and publishers of this website are not liable for any damages or injury resulting from the use or misuse of the information provided on this website.
Endometriosis is a complex and often misunderstood condition that can have a significant impact on quality of life. Many patients live with symptoms for years before receiving clear answers, and it is common to feel uncertain or frustrated during the diagnostic process.
This fact sheet explains what an endometriosis ultrasound assessment involves, why it is performed, and how it fits into diagnosis and treatment planning. In this article, Jacqui, Lead Gynaecological Sonographer at QUFW, talks you through what to expect from your assessment, the different types of endometriosis, and why specialised imaging plays such an important role.
Medical disclaimer: The information in this article is general in nature and provided for educational purposes only. It does not replace medical advice, diagnosis, or treatment. Please consult your doctor or specialist for personalised care.
Endometriosis is a condition where tissue similar to the lining of the uterus grows outside the uterus. These implants can attach to the ovaries, fallopian tubes, bowel, bladder, and other pelvic or abdominal structures.
“Endometriosis is a condition where tissue similar to the lining of the uterus grows outside the uterus,” Jacqui explains in the above video.
Like the uterine lining, this tissue responds to hormonal changes during the menstrual cycle.
“Just as the lining of the uterus thickens and bleeds every month during menstruation, so does this tissue.”
Because the blood and inflammatory fluid cannot drain away normally, this process leads to inflammation, swelling, scarring, and pain.
Ultrasound image of an endometrioma in the left ovary
What are the symptoms of endometriosis?
Endometriosis affects up to one in seven women.
Symptoms vary widely.
“Some people have no pain at all, while others have debilitating symptoms,” says Jacqui.
Common symptoms include:
Painful periods
Chronic pelvic pain
Pain during or after sexual intercourse
Painful bowel motions during menstruation
Abnormal bleeding
Pain with urination
Pain with ovulation
Fatigue
About 30% of patients with endometriosis experience infertility, and symptoms do not always correlate with disease severity.
Why is endometriosis diagnosis often delayed?
In Australia, the average diagnostic delay for endometriosis is approximately 6.4 years.
“Period pain is often dismissed as normal,” Jacqui explains.
Other contributing factors include:
Misdiagnosis at GP or imaging level
Limited access to specialised imaging
Long public hospital surgical waitlists
A shortage of surgeons trained in deep endometriosis surgery
What are the different types of endometriosis?
There are three recognised types of endometriosis, each with different imaging features and clinical implications.
Endometriomas
Endometriomas, often called chocolate cysts, are cysts that form on the ovaries.
“They occur in around 17 to 44% of patients with endometriosis,” Jacqui explains.
They are usually visible on transvaginal ultrasound and act as a warning sign that further assessment of the pelvis is needed.
Superficial endometriosis
Superficial endometriosis accounts for around 80% of cases and involves small lesions on the peritoneal surface.
“Superficial endometriosis is the most subtle form of the disease,” says Jacqui.
Although difficult to detect, advancements in ultrasound technology now enable our team to sometimes directly visualise superficial endometriosis. This is a huge leap forward in the diagnosis of the condition.
Also, while a negative transvaginal scan doesn’t reliably confirm the absence of the disease, a positive transvaginal scan for superficial endometriosis may facilitate a non-invasive diagnosis which may ensure early treatment, prevent progression, and improve outcomes.
“Some women with superficial endometriosis may have more severe symptoms than those with deep endometriosis, Jacqui says”
Deep endometriosis
Deep endometriosis is now considered to be any invasion beyond the peritoneal surface.
“It causes scarring and adhesions that can distort normal anatomy,” Jacqui explains.
It affects 15 to 30% of patients and commonly involves:
Uterosacral ligaments
Posterior vaginal wall
Bowel
Bladder
It is important to understand the difference between superficial endometriosis and deep endometriosis. The latest consensus is that superficial endometriosis should be characterised as a disease that lines the surface of the peritoneum. Any invasion beyond the peritoneal surface is considered deep endometriosis.
What is adenomyosis and its relationship to endometriosis?
Adenomyosis is a separate but related condition where endometrial tissue grows into the muscle wall of the uterus.
“It is commonly diagnosed in women between 40 and 60, however it has been confirmed in younger women,” says Jacqui.
Symptoms often include heavy and painful periods, and adenomyosis frequently coexists with endometriosis.
How is an endometriosis ultrasound performed?
Your assessment begins with a detailed gynaecological history.
First, a transabdominal ultrasound is performed with a full bladder to assess the pelvis and kidneys. This scan provides an overview but does not show deep endometriosis in detail.
“The main endometriosis assessment is performed transvaginally,” Jacqui explains.
The internal scan uses a slender probe with a sterile cover. With your consent, it is gently inserted after you empty your bladder.
During the scan:
The probe is angled carefully to assess pelvic structures
Gentle pressure may be applied to assess organ mobility
The uterus, ovaries, bowel, bladder, and ligaments are examined
“The entire ultrasound assessment takes about 30 minutes and follows well-established protocols.”
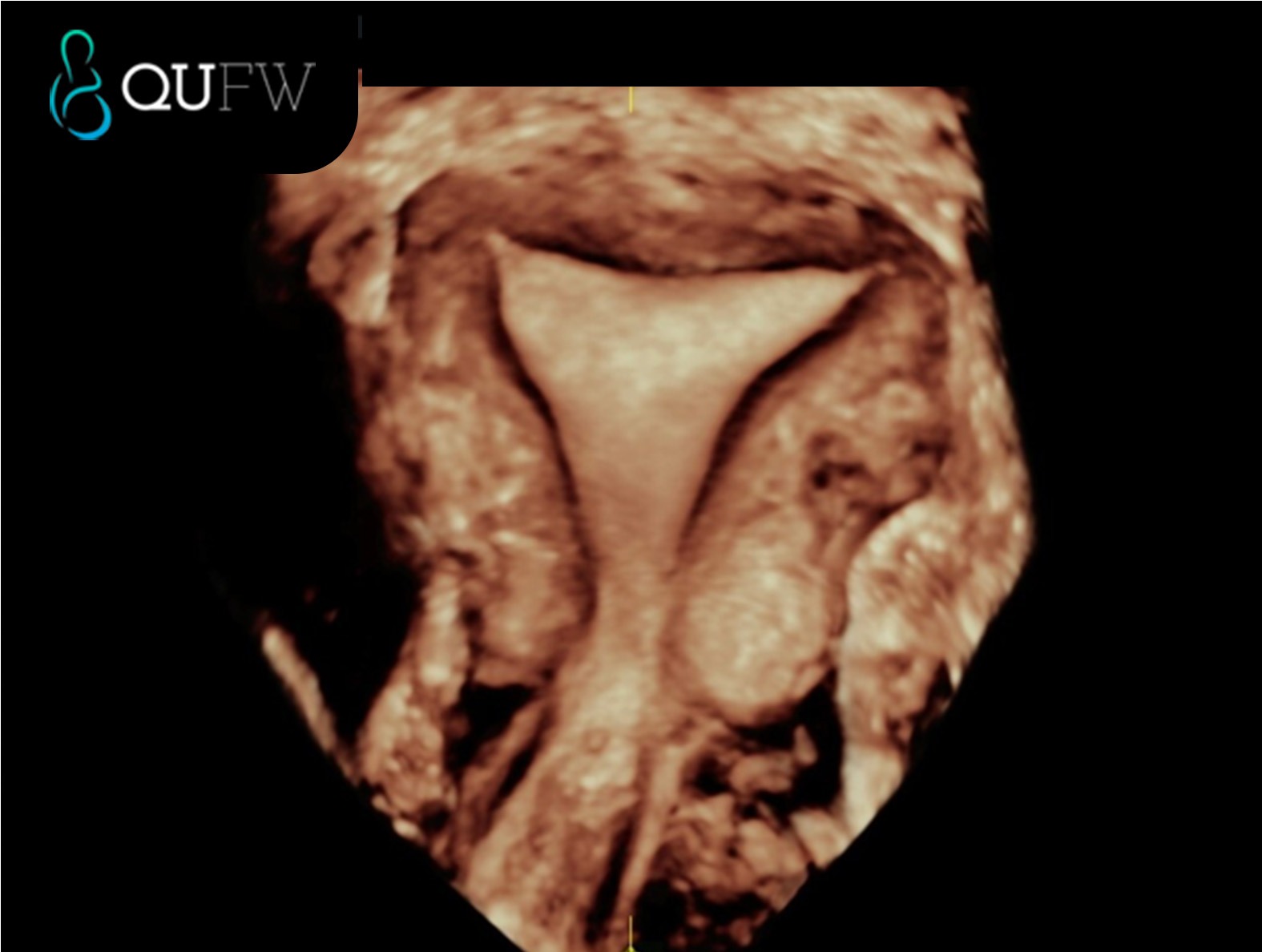
3D reconstructed coronal image of the uterus
What will I feel during and after an endometriosis scan?
Some patients experience tenderness during the examination, particularly if endometriosis is present.
“Some women may not be able to tolerate a transvaginal scan due to intense pain,” Jacqui notes.
Options to support comfort include:
Pain relief before the appointment
Pelvic floor physiotherapy for relaxation techniques
After the scan, mild pain or spotting can occur and usually settles quickly.
“It’s also common to feel emotional after receiving an endometriosis diagnosis,” Jacqui explains.
Ultrasound, MRI, and laparoscopy: how they compare
MRI can be used when a transvaginal scan is not tolerated, but it has limitations.
“MRI is not a dynamic study and cannot assess whether the pelvic organs are stuck together,” Jacqui explains.
Laparoscopy remains a treatment tool but is no longer required purely for diagnosis when high-quality ultrasound is available.
Book your gynaecology scan at QUFW
Living with suspected endometriosis can feel isolating, especially when answers have taken years to find. Many patients describe relief when their pain is finally taken seriously, even if the path forward still feels uncertain.
At QUFW, gynaecology scans are designed to provide clarity, validation, and accurate information to support your care. Your assessment is performed using specialised protocols and interpreted by clinicians with advanced expertise in gynaecological ultrasound and endometriosis. Contact us here.
The goal is to give you and your healthcare team the information needed to make informed decisions about next steps, whether that involves ongoing monitoring, medical management, or surgical planning.
We are here for you.
References
Guerriero, S., Condous, G., van den Bosch, T. et al. (2016). Systematic approach to sonographic evaluation of the pelvis in women with suspected endometriosis. Ultrasound in Obstetrics & Gynaecology, 48(3), 318–332. https://obgyn.onlinelibrary.wiley.com/doi/10.1002/uog.15955
Nisenblat, V., Bossuyt, P. M., Shaikh, R. et al. (2016). Blood biomarkers for the non-invasive diagnosis of endometriosis. Cochrane Database of Systematic Reviews, Issue 5. https://pubmed.ncbi.nlm.nih.gov/27132058/
Transcript
Hi, my name’s Jacqui. I’m the lead gynaecological sonographer for QUFW, and I’m here to talk you through your endometriosis assessment.
Endometriosis is a condition where tissue similar to the lining of the uterus grows outside the uterus. It commonly attaches to the ovaries, fallopian tubes, bowel, and bladder, as well as other organs. Just as the lining of the uterus thickens and bleeds every month during menstruation, so does this tissue. This causes inflammation, swelling, and pain in these areas.
Endometriosis affects as many as one in seven women and people assigned female at birth. Some people have no pain at all, while others have debilitating symptoms such as pain during periods, chronic pelvic pain, pain with sexual intercourse, painful bowel motions during menstruation, abnormal bleeding, pain with urination, pain with ovulation, and fatigue. About 30% of patients with endometriosis experience infertility. In Australia, the average person with endometriosis experiences a diagnostic delay of about 6.4 years.
Why is there a delay in diagnosis?
Period pain is often dismissed as normal. There is also frequent misdiagnosis at the GP level, during imaging, or even at laparoscopy. Public hospital waitlists for surgery can be long, and there are not enough trained surgeons to perform specialised deep endometriosis surgery. There are also limited numbers of trained sonographers to perform advanced endometriosis ultrasounds, and not enough specialists able to accurately report these assessments.
There are three types of endometriosis. The first type is endometriomas, the second is superficial endometriosis, and the third is deep endometriosis.
Endometriomas, also known as chocolate cysts, occur in around 17 to 44% of patients with endometriosis. They can vary in size and may appear on one or both ovaries. They are a warning sign that calls for a thorough investigation of the entire pelvis and are usually easy to see on transvaginal ultrasound.
Superficial endometriosis is the most subtle form of the disease and accounts for about 80% of cases. Ultrasound can sometimes give indications of superficial endometriosis when there is tenderness in a particular area or when the organs appear stuck. In the past, ultrasound had limited sensitivity in detecting superficial endometriosis because the lesions are small and have little volume. However, with ongoing research, we are beginning to see both direct and indirect features of this type. Some women with superficial endometriosis may have more severe symptoms than those with deep endometriosis.
Deep endometriosis is defined as lesions that extend more than five millimetres beneath the peritoneum. It causes scarring and adhesions that can distort normal anatomy. Deep endometriosis accounts for 15 to 30% of cases and is often found on the posterior vaginal wall behind the cervix, the uterosacral ligaments, the bowel, and the bladder. It’s less frequently seen on the ureters, diaphragm, or in surgical scars.
Adenomyosis is another benign gynaecological condition, commonly diagnosed in women between the ages of 40 and 60. It occurs when endometrial tissue grows into the muscle wall of the uterus. Common symptoms include painful and heavy periods. Endometriosis and adenomyosis can often occur together.
How is the ultrasound performed?
First, your gynaecological history is taken. Then a transabdominal scan is performed while your bladder is full. This gives us an overview of your pelvis and allows us to assess your kidneys. The transabdominal scan will not provide detailed information about deep endometriosis.
The main endometriosis assessment is performed transvaginally, using an internal probe that functions like a slender camera. For your comfort and to optimise our views, you’ll be asked to empty your bladder before the internal scan. A sterile probe cover is used, and with your consent, the probe is gently inserted into the vagina.
During the examination, the probe is moved at different angles, and the sonographer may place a hand on your abdomen to apply light pressure and assess the mobility of your uterus and ovaries. The entire ultrasound assessment takes about 30 minutes and follows well-established protocols. The results are often discussed with you, and the report will be sent to your referring doctor in a timely manner.
If you have never had penetrative sexual intercourse or used tampons, a transvaginal scan is still possible with a skilled sonographer and your consent. Some patients experience tenderness, so options include taking pain relief before the appointment. Pelvic floor physiotherapists can also help with relaxation techniques.
Some women, however, may not be able to tolerate a transvaginal scan due to intense pain. In these cases, MRI can be used as an alternative. However, MRI is not a dynamic study and cannot assess whether the pelvic organs are stuck together due to adhesions from endometriosis.
After the transvaginal examination, some women can experience mild pain, which is considered normal. Occasionally, the examination may temporarily increase your pain, but this usually resolves after the ultrasound. Pain relief can be used to ease any discomfort. Some women may also experience light spotting.
It’s also common to feel emotional after receiving an endometriosis diagnosis. Some women feel relieved that their pain has been validated, while others may feel disappointed if the ultrasound appears normal. A normal ultrasound performed by a trained specialist does not rule out all endometriosis. Ultrasound has limitations in diagnosing superficial endometriosis, which is the most common type, affecting about 80% of patients.
The severity of the disease does not always match the severity of symptoms. Some women with superficial endometriosis have more severe pain than those with deep endometriosis. If symptoms cannot be managed, a laparoscopy may be necessary.
If you already have symptoms of endometriosis, do you still need an ultrasound before surgery?
Yes. The aim is to reduce unnecessary surgery, which can cause scarring, adhesions, and further damage to the pelvic organs. The presence of bowel or deep endometriosis suggests that an advanced laparoscopic surgeon should perform the operation rather than a general laparoscopic surgeon.
A transvaginal ultrasound has been shown to have higher sensitivity in detecting deep endometriosis compared to diagnostic laparoscopy. This non-invasive approach allows the disease to be mapped and may reduce the need for diagnostic surgery and surgical surprises.
If you’ve already had an ultrasound that confirms endometriosis, do you need surgery to confirm your diagnosis?
No. A transvaginal ultrasound is an accurate, non-invasive diagnostic tool. There’s no need to confirm the findings with a laparoscopy. If endometriosis is identified on your ultrasound, it gives you and your healthcare team more accurate information to plan your treatment. This may involve surgical removal of endometriosis or non-surgical management.
What is the difference between a standard pelvic ultrasound and a specialised endometriosis assessment?
A standard pelvic ultrasound assesses the uterus and ovaries. This routine scan can detect endometriomas but often misses deep endometriosis affecting structures outside the uterus.
A specialised endometriosis assessment goes beyond these areas to examine the bowel, bladder, and supporting ligaments in both the anterior and posterior compartments. If these areas are not assessed, deep endometriosis may not be detected.
A specialised endometriosis ultrasound is performed by trained specialists using dynamic techniques to assess for organ mobility and adhesions. This method can detect deep endometriosis with high accuracy and sometimes superficial disease as well.
At QUFW, your specialised endometriosis assessment is performed and reported by an expert-trained gynaecologist with advanced skills in interpreting all aspects of endometriosis on ultrasound.
We are here for you.
====================
Content Disclaimer
The information provided on this website is for educational and informational purposes only. It is not intended as a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your obstetric doctor or other qualified provider with any questions you may have regarding a medical condition or treatment and before undertaking a new healthcare regimen.
The content on this website is not intended to be a comprehensive source of information on any particular topic and should not be relied upon as such. The authors and publishers of this website are not liable for any damages or injury resulting from the use or misuse of the information provided on this website.
A gynaecological ultrasound is a safe and effective way to assess the uterus, ovaries, and surrounding pelvic structures. It is commonly requested to investigate symptoms such as pelvic pain, abnormal bleeding, fertility concerns, or to check the position of an intrauterine device.
This guide explains some of the more common pelvic conditions that may be identified during a gynaecological ultrasound and what they may mean for you.
Please note:The information in this article is general in nature and provided for educational purposes only. It does not replace medical advice, diagnosis, or treatment. Please consult your GP or specialist for personalised care.
Conditions commonly identified on gynaecological ultrasound
Endometrial thickness
The endometrium is the lining of the uterus. Its appearance and thickness change throughout the menstrual cycle, becoming thicker after ovulation and thinner after a period. In post-menopausal women, the endometrium is usually much thinner.
Measuring endometrial thickness helps assess causes of abnormal bleeding, hormonal influences, and response to medications. A thickness outside the expected range does not automatically mean something is wrong, but it may prompt further investigation depending on age, symptoms, and medical history.
Fibroids
Fibroids are common, benign growths arising from the muscular wall of the uterus. They vary widely in size, number, and location, and many women are unaware they have them.
Depending on their position, fibroids may contribute to heavy or prolonged periods, pelvic pressure, pain, or fertility concerns. Ultrasound helps map fibroids accurately, which assists doctors in determining whether monitoring, medical management, or further treatment is appropriate.
Endometrial polyps
Endometrial polyps are localised overgrowths of the uterine lining. They are usually benign and can vary in size from a few millimetres to several centimetres.
Polyps may cause irregular bleeding, spotting between periods, or bleeding after menopause. Ultrasound helps identify suspected polyps and assess their size and attachment, supporting decisions about further testing or removal if symptoms are present.
Müllerian anomalies
Müllerian anomalies are congenital differences in the shape or structure of the uterus that develop before birth. Examples include a septate uterus or a bicornuate uterus.
Many women with these variations have no symptoms and only discover them during imaging. In some cases, these anomalies may affect menstruation, fertility, or pregnancy outcomes. Ultrasound plays an important role in identifying uterine anatomy and guiding further assessment if needed.
At QUFW, 3D ultrasound will be used to assess the uterine cavity for Mullerian anomalies. All of our machines at QUFW have 3D capabilities.
Adenomyosis
Adenomyosis occurs when tissue similar to the endometrium grows within the muscular wall of the uterus. This can cause the uterus to appear enlarged or irregular.
It is often associated with heavy periods, painful periods, or chronic pelvic discomfort. Ultrasound looks for specific features that suggest adenomyosis, although findings can be subtle and may overlap with other conditions. Specialist imaging experience improves detection and reporting. Adenomyosis is commonly seen between 40-60 but has been confirmed in younger women.
IUCD (Mirena) placement
Ultrasound is commonly used to assess the position of an intrauterine contraceptive device, such as a Mirena, especially if symptoms like pain or abnormal bleeding occur.
A correctly positioned device sits within the uterine cavity. Ultrasound can identify displacement, embedment, or expulsion. This information helps your doctor decide whether the device can remain in place or needs adjustment or replacement.
Polycystic ovarian morphology (PCOM)
PCOM refers to an ovarian appearance characterised by multiple small follicles arranged around the ovary. This is a descriptive ultrasound finding rather than a diagnosis.
Many women with PCOM have no symptoms and normal hormone levels. PCOM is only one feature considered when assessing for polycystic ovary syndrome (PCOS). A diagnosis of PCOS requires clinical symptoms and blood tests in addition to ultrasound findings.
Ovarian cysts
Ovarian cysts are fluid-filled sacs that can develop as part of the normal menstrual cycle. Most are functional cysts that resolve without treatment.
Ultrasound helps classify cysts based on their appearance, size, and internal features. Some cysts may require follow-up imaging, while others may explain pelvic pain or discomfort. The majority of ovarian cysts are benign.
Superficial endometriosis
Superficial endometriosis involves small deposits of endometrial tissue on the surface of pelvic organs. These deposits are often too small to be directly seen on ultrasound.
Even when superficial endometriosis is not visible, ultrasound can assess pelvic anatomy and exclude other causes of symptoms. Imaging findings are considered alongside clinical history, particularly pain patterns and response to treatment. Learn more about endometriosis here.
Ultrasound image of an endometrioma in the left ovary
Deep endometriosis
Deep endometriosis occurs when endometrial tissue grows deeper into pelvic structures, such as ligaments, bowel, bladder, or uterosacral regions. Any invasion beyond the peritoneal surface can be considered as deep endometriosis.
Specialist gynaecological ultrasound techniques allow targeted assessment of areas commonly affected. Identifying deep endometriosis helps guide management decisions, surgical planning, and referral to appropriate specialists. Learn more about endometriosis here.
Pelvic adhesions
Adhesions are bands of scar tissue that can form following surgery, infection, or inflammation. They may restrict normal movement of pelvic organs.
Adhesions are not always directly visible on ultrasound, but reduced organ mobility or altered anatomy can suggest their presence. Symptoms vary and may include pain, discomfort, or fertility concerns, while some women experience no symptoms at all.
What happens after your ultrasound
Your ultrasound report is sent to your referring doctor, who will discuss the findings with you. Some results require no action, while others may lead to monitoring, further imaging, or referral to a specialist.
Reassurance and next steps
Many pelvic findings are common and manageable. A normal ultrasound is also a frequent and reassuring outcome. When something is identified, it does not always mean treatment is required.
Your healthcare team will guide you through the results and discuss the most appropriate next steps for your situation.
====================
Content Disclaimer
The information provided on this website is for educational and informational purposes only. It is not intended as a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your obstetric doctor or other qualified provider with any questions you may have regarding a medical condition or treatment and before undertaking a new healthcare regimen.
The content on this website is not intended to be a comprehensive source of information on any particular topic and should not be relied upon as such. The authors and publishers of this website are not liable for any damages or injury resulting from the use or misuse of the information provided on this website.
An exciting announcement from QUFW’s founders, Assoc. Prof. Robert Cincotta and Dr. Jackie Chua
“We are delighted to announce the opening of QUFW Toowoomba, our newest obstetrics and gynaecological ultrasound practice, located at the 201a, Level 2, Medici Medical Centre, 15 Scott St, East Toowoomba.
This new location represents another significant step in QUFW’s ongoing commitment to making high-quality ultrasound care more accessible to women and families across southern Queensland.
As part of this exciting development, QUFW has acquired the sonography practice Women’s Health Only Ultrasound, strengthening our local presence and ensuring continuity of care for patients in the region. QUFW remains independently owned and operated.
We are also thrilled to welcome Mary-Louise Barnes, formerly of Women’s Health Only Ultrasound, to the QUFW family. Mary-Louise brings extensive experience and a special interest in obstetrics ultrasound, in particular tertiary imaging.. She will be joined by Allison Mander, an accomplished sonographer with a special interest in gynaecological ultrasound, in particular endometriosis assessment. Together, they form a skilled and compassionate team dedicated to delivering the standard of care that QUFW is known for.
All scans performed at QUFW Toowoomba will be reported by QUFW’s existing team of doctors, maintaining the same high level of diagnostic quality, accuracy, and care that our patients and referring clinicians have come to expect.
The addition of QUFW Toowoomba strengthens our ability to support both patients and referring clinicians throughout the Darling Downs. This expansion marks an important milestone in our mission to provide expert, patient-centred ultrasound services across Queensland.
We look forward to welcoming patients from 24 November 2025 and invite our community to follow our growth as we continue to expand women’s imaging services in regional centres.”
Rob and Jackie
QUFW Toowoomba
201a/ Level 2
Medici Medical Centre
15 Scott St, East Toowoomba, QLD 4350
For more information or to book an appointment, please call 07 4542 7855
Non-invasive prenatal testing (NIPT) has become an important part of early pregnancy care, giving parents insight into their baby’s chromosomes through a simple blood test. But even if NIPT has been done, the 13 week ultrasound is still essential. For parents, it offers a first real look at how the baby is physically developing: seeing the heartbeat, movements, and early features that blood tests alone can’t show. For clinicians, this scan provides anatomical and placental information that NIPT cannot detect, such as structural abnormalities, growth patterns, and chorionicity in multiple pregnancies. Together, NIPT and ultrasound form a more complete picture, combining genetic information with visible evidence of development and maternal health.
NIPT is a powerful tool, but it has limits. For parents, it’s helpful to know what questions a blood test can answer — and what still requires an ultrasound. For clinicians, understanding the complementary role of each test ensures a balanced approach to screening.
What NIPT does well:
Detects common chromosomal conditions such as Trisomy 21 (Down syndrome), Trisomy 18, and Trisomy 13
Can also check for sex chromosome conditions (depending on the test type)
Provides a high degree of accuracy, reducing the need for some invasive tests
Uses a simple blood sample, posing no risk to the pregnancy
What NIPT doesn’t do:
Does not check the baby’s anatomy or detect structural abnormalities
Cannot show how the placenta is forming or functioning
Cannot confirm growth, heartbeat, or the number of babies
May still require follow-up ultrasound or diagnostic testing if results are high risk
NIPT
13 Week Ultrasound
Analyses cell-free placental DNA in maternal blood
Provides a real-time view of the baby and placenta
Detects chromosomal abnormalities with high sensitivity and specificity
Non-invasive to the pregnancy, no physical risk to the developing fetus
Non-invasive, visual reassurance for parents
Cannot assess physical growth or maternal health risks
Screens for preeclampsia risk and placental development
Often done from 10 weeks onwards
Performed between 13 weeks and 13 weeks 6 days
In practice, NIPT answers questions about chromosomes, while the 13 week ultrasound answers questions about development and health.
2. Key Assessments at 13 Weeks
During the 13 week ultrasound, several important checks are carried out to build a clear picture of how the pregnancy is progressing. The scan confirms the baby’s heartbeat and viability, providing reassurance while also establishing cardiac activity, rhythm, and rate. Growth is measured through the crown–rump length, which is the most accurate way to confirm gestational age and due date between 11 and 14 weeks.
The scan may also determine the number of babies, if not confirmed during an early dating/viability scan, confirming whether it is a single or multiple pregnancy. In multiple pregnancies, chorionicity and amnionicity are identified, which are essential for planning care. Placental development is reviewed, with the location and attachment site documented so any early concerns can be monitored.
Finally, an early anatomy review is performed, allowing a first assessment of the brain, face, heart, spine, abdomen, abdominal wall, limbs, and other structures. While detailed anatomy scans follow later in pregnancy, this early survey can sometimes detect major abnormalities, giving families and clinicians valuable information sooner.
Early structural assessment of the upper limbs
3. Detecting Early Concerns
One of the main strengths of the 13 week ultrasound is its ability to highlight potential issues earlier in pregnancy, giving families more time to understand their options and clinicians more time to plan care.
Areas where concerns may be detected include:
Structural abnormalities such as issues with the brain, face, spine, abdomen, abdominal wall, or limbs
Chromosomal indicators like increased nuchal translucency or absent nasal bone
Placental concerns that could affect growth and development later in pregnancy
Signs of complications in multiple pregnancies, such as unequal sharing of the placenta
Possible Concern
What the Scan May Show
Next Steps
Brain or skull abnormality
Absence of skull bones (acrania), irregular brain structure
Referral for detailed scan, genetic counselling
Facial structures
Absence of the Nasal bone, suggestion of early features of cleft lip/palate, facial development of the orbits
Referral for detailed scan, genetic counselling
Spinal abnormality
Abnormal curvature, incomplete closure of spine
Specialist ultrasound, ongoing monitoring
Abdominal structures
Presence of stomach, diaphragm, bladder, kidneys, 3 vessel cord
Abdominal wall defect
Organs seen outside abdominal cavity as in exomphalos, gastroschisis
Referral to tertiary care, surgical planning
Increased NT or absent nasal bone
Higher chance of chromosomal condition
Further assessment of fetal cardiac structures
Follow-up with NIPT, CVS, or amniocentesis
Further cardiac evaluation in the event that the NT measures >3.5mm and low risk NIPT or normal karyotype has been performed.
Placental issues
Abnormal attachment such as early detection of Placenta Accreta Spectrum.
Monitoring, follow-up scans later in pregnancy
Twin complications
Discordant growth, shared placenta risks
Closer surveillance, specialist input
By identifying these concerns early, the 13 week scan helps guide whether further investigations or specialist referrals are needed. It is not a diagnosis on its own but an important first step in recognising when closer attention may be required.
Early structural assessment of the spine
4. Screening for Maternal Health
The 13 week ultrasound also provides information about the mother’s health and how the pregnancy may progress. A key focus at this stage is the risk of preeclampsia, a condition that can cause high blood pressure and complications later in pregnancy. The scan can be combined with maternal blood pressure readings, blood test results, and medical history to estimate the likelihood of developing preeclampsia. If a higher risk is identified, early interventions such as low-dose aspirin and closer monitoring can be recommended, improving outcomes for both mother and baby.
Placental development is another area of assessment. The position and quality of the placenta are reviewed to ensure it is developing normally and providing adequate support for the pregnancy. Identifying placental issues early helps clinicians plan follow-up care and keep a close watch on the baby’s growth throughout the second and third trimesters.
5. How Results Shape Care
The results of the 13 week ultrasound, especially when considered alongside NIPT, shape how care is managed for the rest of the pregnancy. Together, the two tests provide a comprehensive view: NIPT offers insight into the baby’s chromosomes, while ultrasound shows physical development, placental function, and maternal health factors. This combined approach helps guide decisions about further testing, the need for specialist referrals, and the level of monitoring required.
For parents, this means reassurance that the pregnancy is being tracked with the best tools available, and that potential issues can be identified earlier rather than later. For clinicians, it provides a structured baseline that supports personalised care throughout the pregnancy.
The 13 week ultrasound is therefore much more than a milestone moment to see the baby on screen. It is a pivotal point in early pregnancy care, one that combines emotional connection with medical precision. Used together with NIPT, it ensures families and healthcare providers have the clearest possible picture to support a safe and healthy journey ahead.
====================
Content Disclaimer
The information provided on this website is for educational and informational purposes only. It is not intended as a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your obstetric doctor or other qualified provider with any questions you may have regarding a medical condition or treatment and before undertaking a new healthcare regimen.
The content on this website is not intended to be a comprehensive source of information on any particular topic and should not be relied upon as such. The authors and publishers of this website are not liable for any damages or injury resulting from the use or misuse of the information provided on this website.