QUFW is currently unable to upload ultrasound reports to My Health Record due to a temporary system limitation. In the meantime, all patients will continue to receive a copy of their ultrasound report following their examination, and a copy will also be provided to their referring practitioner. If you would like your ultrasound report to be uploaded to My Health Record once this functionality becomes available, please email [email protected] with your request. We appreciate your patience and understanding and apologise for any inconvenience. — QUFW Management
The 13 week ultrasound is one of the most important early scans in pregnancy. Usually performed between 13 weeks and 13 weeks 6 days, it gives parents a first detailed look at their baby’s growth and development, often providing reassurance as they see the heartbeat, movements, and forming features. At the same time, this scan holds significant clinical value. It marks the end of the first trimester, when crown–rump length measurement is most accurate for dating the pregnancy, nuchal translucency assessment is most reliable, and an early structural survey can detect major anomalies. These combined insights make the 13 week ultrasound both a meaningful milestone for parents and a cornerstone of first trimester screening and early pregnancy care.
The 13 week ultrasound plays a key role in checking that your pregnancy is progressing as expected. It confirms your baby’s heartbeat, measures growth, and if not confirmed in an earlier viability ultrasound can identify whether you are carrying one baby or multiples. Its major purpose is to assess the early anatomical structures that have developed by 13 weeks. The scan can also assess the placenta to check its position is appropriate at this early gestation, however it is important to note that placental position is largely checked at the 20 week morphology assessment. For parents, these checks bring reassurance that things are on track, while for clinicians, they provide vital data for guiding care for the ongoing pregnancy.
At this stage, crown–rump length measurement helps establish accurate gestational age, chorionicity can be determined in multiple pregnancies, and the position of the placenta is documented. Together, these findings set the foundation for monitoring both maternal and fetal health as the pregnancy continues.
2. Early Anatomy Check
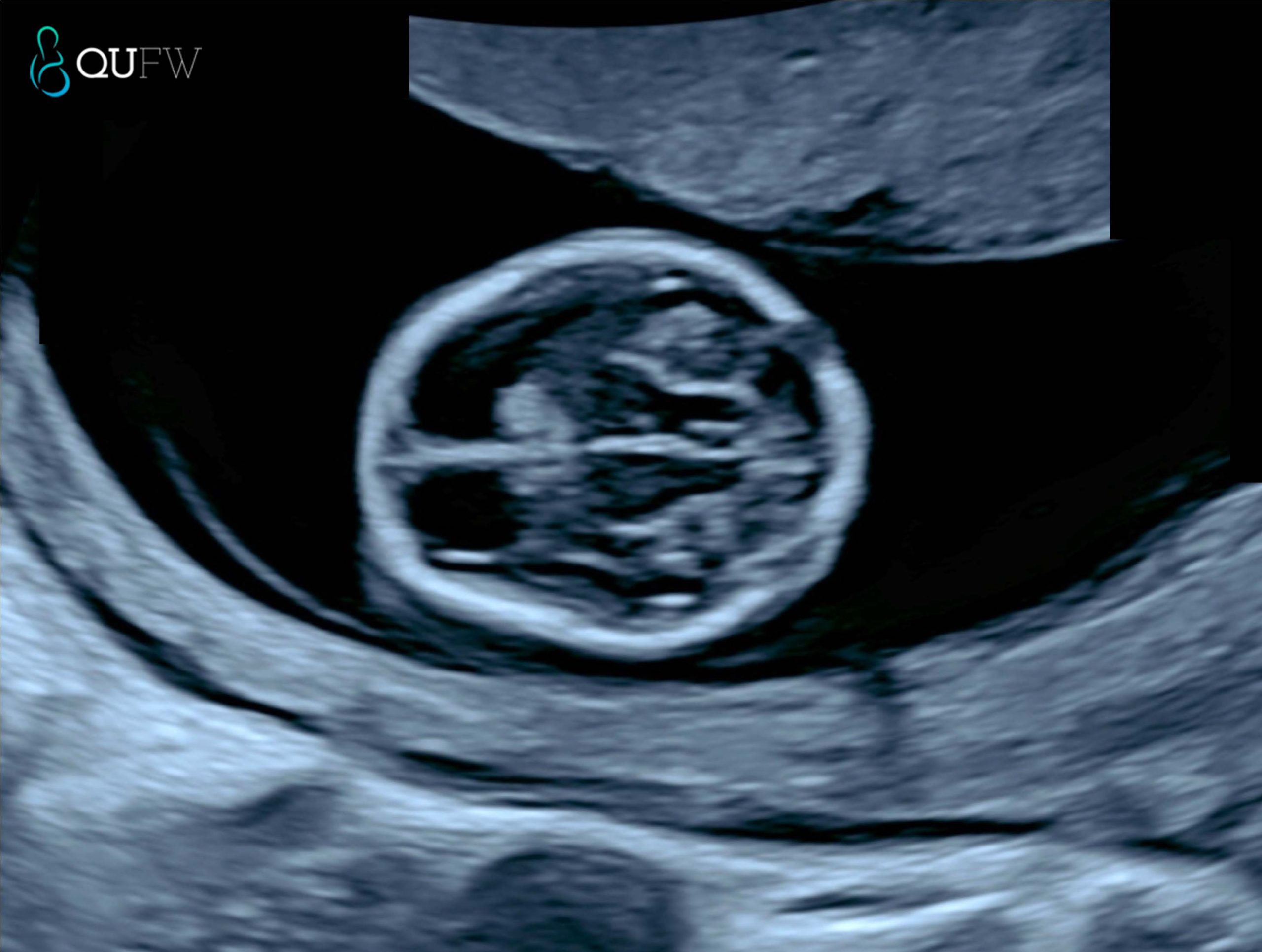
At around 13 weeks, ultrasound technology allows a first look at your baby’s developing anatomy. For parents, this is often the first time you see just how much detail has already formed, including tiny hands and feet, the curve of the spine, and the outline of the brain. For clinicians, this scan provides a systematic review of early structures that can reveal major anomalies at an earlier stage than later pregnancy scans.
Key areas assessed include:
Brain, skull and face – ensuring the skull is formed, the brain appears normal for this gestational age and the early facial structures are developed
Spine – checking alignment and early closure of the neural tube
Heart – confirming rhythm and looking at the early chambers
Abdomen and abdominal wall – ruling out major structures such as diaphragm, stomach, kidneys, bladder and abdominal wall defects
Limbs – confirming presence and movement of arms and legs
What parents see
What clinicians assess
Baby’s profile, head, and movements
Cranial structure, early detection of acrania or anencephaly, early brain development and evidence of early signs of Open Neural Tube Defects (ONTD’s)
Early facial structures and early detection of facial clefts.
Curved spine on screen
Spinal alignment and signs of neural tube defects
Tiny heartbeat flicker
Cardiac rhythm, chamber development
Wriggling arms and legs
Limb formation, detection of limb reduction anomalies
Abdomen outline
Integrity of the abdominal wall, exclusion of exomphalos or gastroschisis
Abdomen
Abdominal structures such as the diaphragm, stomach filling, presence of both kidneys, appropriate bladder filling, evidence of 3 vessel cord and cord insertion.
For parents, these images are a reassuring sign of normal growth. For clinicians, they provide a vital opportunity to detect significant problems early, allowing for referral to specialist care if required.
Early structural assessment of the fetal brain
3. First Trimester Combined Screening – Chromosomal Abnormality Screening
The 13 week ultrasound can also help assess the risk of chromosomal conditions, such as Down syndrome (Trisomy 21), Trisomy 18, and Trisomy 13.
In the absence of NIPT screening, a First Trimester Combined Screening (FTCS) may be performed to provide a risk assessment screening for Trisomy 21, Trisomy 18 and Trisomy 13 by utilising the risk assessment algorithm provided by the Fetal Medicine Foundation. An early anatomy assessment scan is performed at the same time as the FTCS assessment.
In the event that a NIPT screening has been performed, it has been recommended by ISUOG International Society of Ultrasound in Obstetrics and Gynaecology under the consensus statement that “First-trimester risk estimates for trisomies 21, 18 and 13 based on nuchal translucency measurements and maternal biochemistry should not be computed in a woman who has already received a normal NIPT result for these trisomies” (reference here).
The Fetal Medicine Foundation (FMF) algorithm is a first-trimester prenatal screening method for Trisomy 21 (Down Syndrome) that uses maternal age, fetal nuchal translucency (NT) ultrasound measurements, and maternal serum markers (free beta-hCG and PAPP-A) to calculate a risk score. The algorithm helps identify pregnancies at higher risk for Trisomy 21, but it’s a screening tool, not a diagnostic test, and a higher risk score may lead to further invasive tests like amniocentesis or chorionic villus sampling (CVS).
How the FMF Algorithm Works
Maternal Age: Maternal age is a fundamental factor, as the risk of Down Syndrome increases with maternal age.
Ultrasound (NT Measurement): A detailed first-trimester ultrasound is performed to measure the nuchal translucency (NT), a collection of fluid at the back of the fetus’s neck.
Biochemical Markers: Maternal blood is tested for two hormones:
Free beta-hCG (free beta-human chorionic gonadotropin): Typically elevated in Down Syndrome pregnancies.
PAPP-A (pregnancy-associated plasma protein-A): Generally lower in Down Syndrome pregnancies.
Risk Calculation: The FMF algorithm combines these factors to generate a personalised risk for Trisomy 21, Trisomy 18 and Trisomy 13.
For parents, this part of the scan offers important reassurance or an early signal that further testing may be needed. For clinicians, it provides measurable markers that contribute to first-trimester combined screening.
Markers typically assessed at this stage include:
Nuchal translucency (NT): a fluid space at the back of the baby’s neck that, if increased, can indicate a higher chance of chromosomal abnormality.
Nasal bone: its presence or absence can be a significant marker in risk assessment.
Ductus venosus flow: abnormal flow patterns may be associated with aneuploidy or cardiac defects.
Tricuspid regurgitation: when present, it can increase the risk profile.
For parents
For clinicians
The scan looks at small features, like the fluid behind the baby’s neck and nose bone, that can indicate a higher or lower chance of conditions such as Down syndrome.
NT is measured between 11+0 and 13+6 weeks when CRL is 45–84 mm; when combined with maternal serum biochemistry (free β-hCG, PAPP-A), this forms the basis of first-trimester combined screening.
It is preferred at QUFW to perform this assessment between 13 weeks and 13+6 days
A higher-than-expected NT doesn’t mean something is wrong, but it may lead to follow-up testing for clarity particularly for congenital heart defects or other genetic syndromes.
Integration of ultrasound markers with serum and maternal age yields detection rates of >90% for Trisomy 21 at a 5% false-positive rate.
In the event of an NT measurement >3.5mm, further structural assessment of the fetus including the heart for congenital heart defects is made as part of the early anatomy scan.
Results can help guide whether additional tests, such as NIPT or diagnostic procedures (CVS, amniocentesis), are recommended.
In practice, this means the 13 week scan is more than just a “look at the baby” moment. It forms a crucial part of early screening that combines visual markers, blood tests, and clinical context to give the clearest picture possible at this stage of pregnancy.
Nuchal translucency assessment
4. Maternal Health Screening
The 13 week ultrasound is not only about checking the baby, it also provides valuable information about the mother’s health. For parents, this means doctors can look for early signs of conditions that could affect the pregnancy, helping to keep both mother and baby safe. For clinicians, this scan offers an opportunity to assess maternal risk factors and build a plan for ongoing care.
One of the key conditions that can be screened for is preeclampsia, a complication that can lead to high blood pressure and other serious health issues later in pregnancy. At this stage, the scan can be combined with blood pressure readings, maternal history, and blood test results to estimate a woman’s risk. If the risk is found to be higher, preventive steps can be started early.
The scan may also highlight placental concerns. Early assessment of how the placenta is developing and where it is attached provides important insight into how well it might support the pregnancy. These checks give reassurance to parents while helping clinicians take proactive measures if any issues are identified
====================
Content Disclaimer
The information provided on this website is for educational and informational purposes only. It is not intended as a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your obstetric doctor or other qualified provider with any questions you may have regarding a medical condition or treatment and before undertaking a new healthcare regimen.
The content on this website is not intended to be a comprehensive source of information on any particular topic and should not be relied upon as such. The authors and publishers of this website are not liable for any damages or injury resulting from the use or misuse of the information provided on this website.
In early pregnancy, you might hear a range of terms used for the scans you might need, such as “viability,” “dating,” “early anatomy,” or “NIPT.” These names can sound similar, and it’s not always clear how they differ or when each one is recommended.
This fact sheet explains the different types of early pregnancy scans so you can understand their purpose and timing. It answers the following questions:
In the first trimester, ultrasound can confirm pregnancy, check wellbeing, and estimate due dates.
Common scans include:
Viability and Dating scan – a viability scan or a dating scan refer to the same thing and involve an early check of pregnancy location and heartbeat. The Sonographer measures the fetus to establish or confirm an estimated due date (EDD)
Early Anatomy scan – assesses early anatomy and screens for certain structural conditions
First Trimester Combined Screening scan – this scan is the same as the Early anatomy scan but provides additional screening for chromosomal abnormalities, particularly Trisomy 21, 18 and 13. The risk assessment is only performed if the patient has not had a NIPT performed. The NIPT has a higher detection rate for Trisomy 21 (almost 99% detection rate) as opposed to approximately 90% detection rate.
NIPT (non-invasive prenatal testing) – blood test for chromosomal screening, recommended to be accompanied alongside a viability ultrasound.
Here’s a breakdown of each of these scans:
2. Dating and Viability scan (around 6–12 weeks)
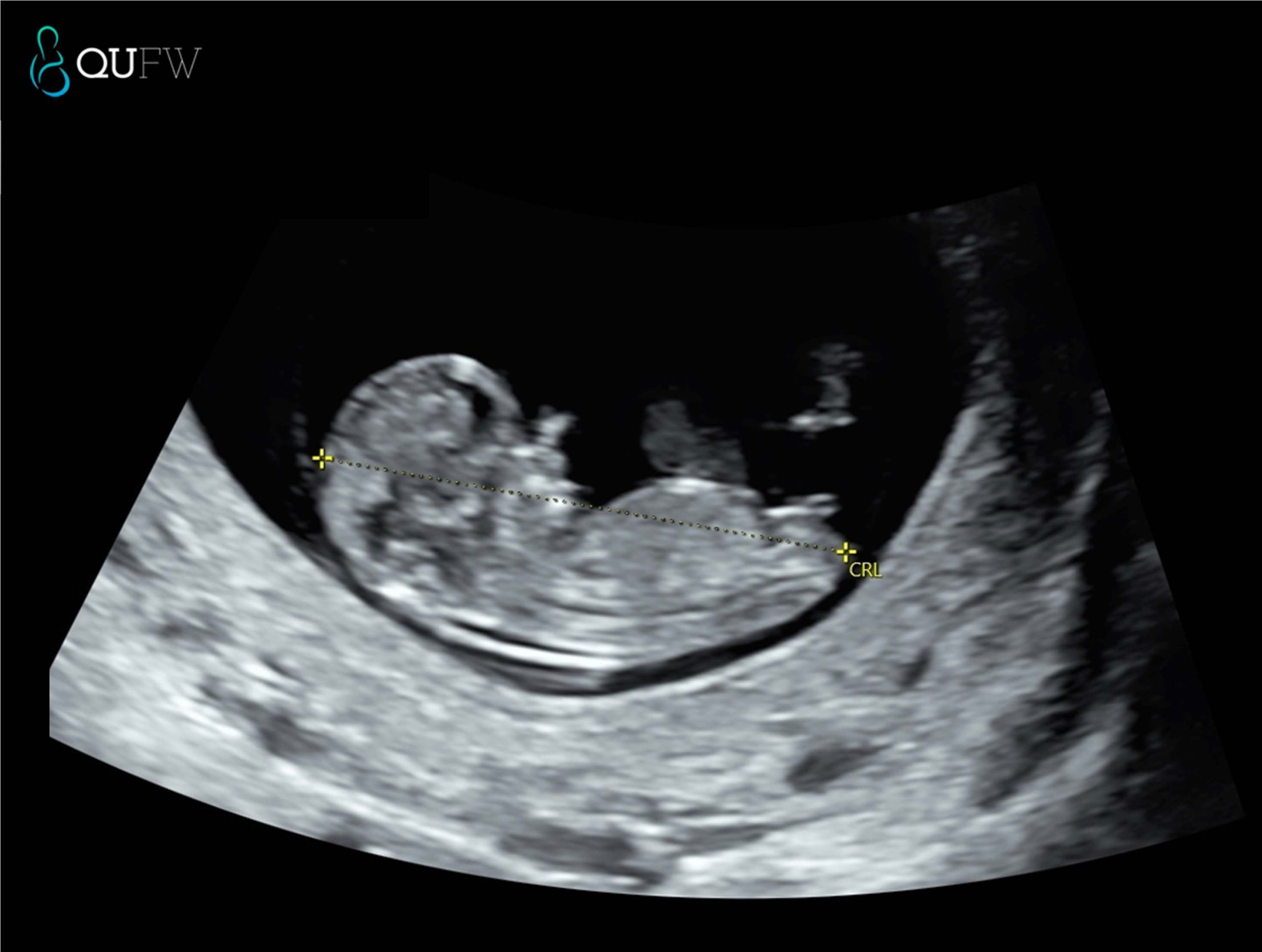
A viability scan confirms that the pregnancy is in the uterus, checks for a heartbeat, and assesses early development. A dating scan measures the crown–rump length (CRL) to estimate gestational age and your EDD. This timing offers a high degree of accuracy (± 5 days). You may be referred for a viability scan if you:
Have pain or bleeding
Have had an ectopic pregnancy before
Conceived via IVF
Have a history of pregnancy loss
It also confirms:
The baby’s heartbeat
Whether you are carrying one baby or multiples
The pregnancy location
If performed very early (before 6 weeks), it may be too soon to see a heartbeat, and a repeat scan may be needed.
Dating scan prior to NIPT
3. Early Anatomy scan (13–13+6 weeks)
The Early Anatomy scan assesses early development and screens for specific structural anomalies. At QUFW we also perform a risk assessment for pre-eclampsia at this scan. The early anatomy scan is performed in conjunction with an NIPT. If you elect not to have NIPT then you will be asked if you would like a risk assessment for Trisomy 21, 18 and 13 (the most common chromosomal anomalies) performed in addition to the anatomical assessment, in which case this then becomes a FTCS (see below).
It also checks:
Heartbeat
Cervical length assessment
Placenta position
Multiple pregnancy details
4. If the scan’s EDD differs from your LMP-based date, your healthcare provider will usually use the ultrasound date.
This is the same as an early anatomy scan, however we provide a risk assessment for chromosomal abnormalities like Trisomy 21, 18, and 13. As a screening for Down Syndrome, it has approx. 90% detection rate when combining the following factors such as
Maternal age and background risk
Ultrasound markers such as nuchal translucency, nasal bone, fetal heart rate
Maternal serum biochemistry (Free beta-hCG and PAPP-A)
At QUFW, similar to the Early Anatomy scan we also perform a pre-eclampsia risk assessment as part of this scan.
Nuchal translucency assessment
5. NIPT and its timing
NIPT is a blood test that can be done from around 10 weeks of pregnancy. At QUFW, we prefer to book NIPT’s from 10 weeks 2 days at the earliest.
It analyses small fragments of the baby’s DNA in the mother’s blood to assess the likelihood of certain chromosomal conditions. NIPT does not replace ultrasound which assesses for structural abnormalities.
6. Which scan should I book first?
It depends on your history and how certain you are of your dates:
Uncertain LMP or irregular cycles – dating and viability scan between 7–12 weeks
History of pregnancy complications – Viability and dating scan from 6 weeks gestation
IVF conception – viability scan at 6–7 weeks, then Early Anatomy scan at 13–13+6 weeks
Known LMP and no risk factors – dating and viability scan between 7-12 weeks, followed by an Early Anatomy scan. Your GP or specialist will recommend a plan suited to your circumstances.
FAQs
Is a viability scan the same as a dating scan?
A viability and dating scan is essentially the same scan and confirms the presence of a pregnancy in the correct location, if it is a multiple pregnancy and confirms that a heart beat is present. It is also used to either confirm or establish correct dating or due date for the pregnancy.
Do I need both Early Anatomy and NIPT?
A NIPT is a screening test for chromosomal abnormalities. It does not detect structural or developmental concerns with the developing fetus. It is advised that an Early Anatomy scan is performed between 13 – 13 weeks 6 days as a structural assessment of your baby. At QUFW we also perform a Preeclampsia screening as a component of the Early Anatomy scan. A low probability result for a NIPT, does not exclude a structural concern in a pregnancy.
When is the best time for a dating scan?
Between 7 and 12 weeks for best accuracy.
Can an Early Anatomy scan detect all conditions?
No. It screens for certain conditions but not all genetic or structural differences may be detected at this early gestation. A further morphology scan is recommended between 20-22 weeks to reassess the baby.
====================
Content Disclaimer
The information provided on this website is for educational and informational purposes only. It is not intended as a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your obstetric doctor or other qualified provider with any questions you may have regarding a medical condition or treatment and before undertaking a new healthcare regimen.
The content on this website is not intended to be a comprehensive source of information on any particular topic and should not be relied upon as such. The authors and publishers of this website are not liable for any damages or injury resulting from the use or misuse of the information provided on this website.
A dating scan is an early pregnancy ultrasound used to measure the developing baby and estimate gestational age. It also confirms the baby’s heartbeat, checks for multiple pregnancies, and verifies the pregnancy location in the uterus.
At QUFW, dating scans are performed by our caring, experienced sonographers using high-resolution equipment to ensure accurate measurement and clear images.
The most accurate time for a dating scan is between 7 and 10 weeks of pregnancy.
Before 7 weeks: The scan can confirm a gestational sac and yolk sac from 5 weeks, a heartbeat after 6 weeks, but measurements may be less reliable to confirm viability and dating A gestational sac visualised within the uterus confirms correct pregnancy location.
Between 7 and 10 weeks: The crown–rump length (CRL) measurement is most accurate for establishing your estimated due date (EDD).
After 10 weeks: Dating is possible, but accuracy decreases as babies start to vary more in size.
Some people have an earlier scan (6–7 weeks) if they have irregular cycles, are unsure of their last menstrual period (LMP), have conceived through IVF, or have a history of pregnancy complications.
8 week fetus with heartbeat
2. What happens during a dating scan?
At QUFW, your sonographer will:
Review your referral and confirm your details.
Explain the scan process and answer any questions.
Perform the scan using either a transabdominal (across the abdomen) or transvaginal (internal) approach, depending on gestational age and image clarity.
Measure the CRL, check for heartbeat, number of babies, and other factors such as ovaries. Provide images and send a detailed report to your referring doctor.
Most dating scans take around 15–30 minutes. They are safe, non-invasive, and use no radiation, however we always practice ALARA (As Low As Reasonably Achievable) principles.
3. How accurate is a dating scan?
A dating scan in the first trimester is a reliable way to determine gestational age.
CRL measurements taken between 7 and 10 weeks are accurate to within ± 5 days.
Later scans may be less accurate because individual growth patterns vary.
If the scan’s EDD differs from your LMP-based date, your healthcare provider will usually use the ultrasound date.
3D image of an 8 week fetus
4. Do I need a dating scan?
You may be advised to have one if:
You are unsure of your LMP or have irregular cycles.
You have conceived via assisted reproduction.
You have a history of early pregnancy loss or ectopic pregnancy.
Your doctor recommends one for clinical reasons.
5. What is the difference between a dating scan and the 13 week early anatomy scan?
While both are first-trimester ultrasounds, their purposes differ:
Dating scan
Early anatomy scan/First Trimester Combined Screening ultrasound
7–12 weeks
13-13+6 weeks
Measures CRL to determine EDD
Measures CRL to confirm EDD and appropriate growth of baby.
Can be used as a dating scan if no prior dating ultrasound has been performed.
Confirms heartbeat, multiples, location of pregnancy
Checks early anatomy structures including a heart beat
In the instance of no prior NIPT, it can provide a First trimester risk assessment for chromosomal abnormalities such as Trisomy 21, 18 and 13 when combined with First trimester blood tests and measuring the fluid at the back of the baby’s neck (Nuchal Translucency)
Can also provide Pre-eclampsia screening
FAQs
Is a dating scan safe?
Yes. Ultrasound is considered safe in pregnancy and does not use radiation.
Can my due date change after a dating scan?
Yes. If ultrasound findings differ from LMP-based dates, your healthcare provider may adjust your due date.
Can a dating scan detect twins?
Yes. A dating scan can confirm if you are carrying more than one baby and whether they share the same placenta or have separate placentas which is important for managing your pregnancy moving forward.
Do I need a full bladder for a dating scan?
For an early dating scan, a partially full bladder may help improve image clarity. Your clinic will confirm preparation instructions when booking.
What if the scan doesn’t show a heartbeat?
If it’s too early in pregnancy, the heartbeat may not be visible yet. Your doctor may recommend repeating the scan in one to two weeks.
Can a dating scan show the baby’s gender?
No. It is too early in pregnancy for accurate gender determination.
====================
Content Disclaimer
The information provided on this website is for educational and informational purposes only. It is not intended as a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your obstetric doctor or other qualified provider with any questions you may have regarding a medical condition or treatment and before undertaking a new healthcare regimen.
The content on this website is not intended to be a comprehensive source of information on any particular topic and should not be relied upon as such. The authors and publishers of this website are not liable for any damages or injury resulting from the use or misuse of the information provided on this website.
Preeclampsia is a pregnancy-related condition that typically develops after 20 weeks. This condition, which affects both mother and baby, is caused by changes in blood pressure and the way the placenta functions. It may lead to symptoms like protein in the urine or complications involving the liver, brain, or blood.
During your pregnancy, a preeclampsia risk assessment may be offered around the time of your 13-week anatomy scan. This screening helps identify women who may benefit from early treatment or closer monitoring.
You might have questions about what it means to be in the “high-risk” category, how accurate the screening is, and whether being high risk means you will definitely develop preeclampsia.
Preeclampsia is a blood pressure syndrome that can affect some women from 20 weeks gestation onwards. It’s a condition unique to pregnancy that involves high blood pressure and signs of stress on other organs such as the kidneys, liver, and brain. One of the earliest indicators can be protein leaking into the urine.
In more serious cases, preeclampsia can lead to complications such as poor growth in the baby, or early delivery. Although these outcomes are rare, they highlight the importance of early detection and careful monitoring.
Preeclampsia is not the same as chronic high blood pressure, although the two can overlap. It develops specifically in pregnancy and usually resolves after birth, but it requires active management to reduce risks for both mother and baby.
Ultrasound of the blood flow through a uterine artery (Transabdominal assessment of the uterine artery Doppler waveform in the first trimester)
2. Who is considered high risk?
A preeclampsia risk assessment helps identify women who may benefit from early intervention. This screening is usually performed during your 13-week ultrasound scan and combines information from your medical history, blood pressure, and specialised tests. It can detect up to 80% of women who may go on to develop early preeclampsia.
The threshold for being classified as “at risk” is low. If your estimated risk is 1% or greater, you will be considered in the high-risk group. This simply means your risk is higher than the background population, not that you will definitely develop the condition.
Factors that increase the chance of being classified as high risk include:
A history of high blood pressure, kidney disease, diabetes, or autoimmune conditions
First pregnancy or a large gap since your last pregnancy
Multiple pregnancy (e.g. twins or triplets)
Assisted conception (e.g. IVF)
Family history of preeclampsia (mother or sisters)
Higher maternal age or elevated BMI
Being labelled high risk can feel concerning, but it allows for preventative strategies and closer follow-up that can improve outcomes.
3. Screening and early detection
Preeclampsia risk screening is usually done at the time of your 13-week anatomy scan. It combines several pieces of information to estimate your individual risk. This includes:
Your medical and pregnancy history
Blood pressure readings
Blood test results (including markers like PAPP-A and PlGF)
Uterine artery Doppler measurements, which assess blood flow to the placenta
This assessment is designed to catch early signs of concern, well before any symptoms appear. If your risk is calculated at 1% or more, your care team may recommend starting preventative treatment.
It’s important to remember that the risk estimate is not a diagnosis. Many women identified as high risk go on to have healthy pregnancies without developing preeclampsia. The aim of early detection is to personalise care and reduce the likelihood of complications through early intervention.
4. Preventative measures
If you are identified as high risk for preeclampsia, your doctor may recommend starting preventative treatment early in pregnancy. One of the most effective measures is low-dose aspirin.
Research from the ASPRE trial shows that taking 150 mg of aspirin each night, started between 11 and 14 weeks of pregnancy, can reduce the risk of preterm preeclampsia by approximately 62%. It may reduce the risk of very early preeclampsia (before 34 weeks) by even more, though this comes from subgroup analyses rather than the primary trial result. Aspirin is usually taken at night, and most women will be advised to continue until between 34 and 36 weeks of pregnancy.
This dose is considered safe in pregnancy unless you have a known allergy or a medical reason not to take it. Always check with your doctor or midwife before starting, including about the correct tablet formulation for your situation.
5. Monitoring and management
If you are considered high risk for preeclampsia, your pregnancy care will usually include closer monitoring to detect any early changes. This may involve:
Frequent blood pressure checks
Urine testing for protein
Regular blood tests to monitor kidney and liver function
Ongoing growth scans to assess your baby’s development and placental function
Your care team will look for early signs that the condition may be developing so that timely decisions can be made. If preeclampsia is confirmed, medication may be prescribed to help control blood pressure.
In some cases, hospitalisation is needed, particularly if the condition worsens or your baby is not growing well. The goal is to continue the pregnancy safely for as long as possible, while reducing the risk of complications.
Monitoring helps your care team balance the needs of both mother and baby, aiming to optimise outcomes while planning the safest timing and mode of delivery.
6. Conclusion
Being identified as high risk for preeclampsia can be unsettling, but it provides an opportunity for early intervention and tailored care. With screening available from 13 weeks of gestation, many women at increased risk can benefit from proven preventative measures like low-dose aspirin.
Regular monitoring, growth scans, and blood pressure checks will help your care team manage your pregnancy safely. Most women in the high-risk category go on to have healthy pregnancies and births.
If you have questions about your risk, screening results, or treatment options, speak with your doctor.
7. Video transcript
This is some information about your preeclampsia risk assessment and what it means if you are high risk. Preeclampsia is a blood pressure syndrome of pregnancy that can affect some women from 20 weeks gestation onwards. It causes high blood pressure, leaking protein in the urine and changes in the blood, brain and liver. In some rare cases. This can result in baby being small or born prematurely. Preeclampsia risk assessment identifies up to 80% of women who may develop this condition early. This risk assessment is performed at the time of your 13 week anatomy scan. It’s important to understand that we have a very low threshold for identifying someone at increased risk. If your risk is 1% or higher, you will fall into the at risk group. At risk means higher than the background population, but it certainly does not mean you will definitely develop the condition. It has been shown that starting aspirin before 16 weeks of pregnancy can reduce the chance or delay the onset of developing preeclampsia by up to 80%. The dose of aspirin recommended is 150 milligrams. This is half of a 300 milligram tablet. It’s best taken at nighttime every night until you are between 34 and 36 weeks gestation. This dose is considered safe, providing of course that you have no allergies or medical issues that prevent you from taking aspirin. Please check with your doctor to confirm that they are happy for you to commence aspirin. If you have any vaginal bleeding after commencing the aspirin, we recommend you cease its use and speak to your doctor for further advice.
====================
Content Disclaimer
The information provided on this website is for educational and informational purposes only. It is not intended as a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your obstetric doctor or other qualified provider with any questions you may have regarding a medical condition or treatment and before undertaking a new healthcare regimen.
The content on this website is not intended to be a comprehensive source of information on any particular topic and should not be relied upon as such. The authors and publishers of this website are not liable for any damages or injury resulting from the use or misuse of the information provided on this website.
A morphology scan is an exciting and important part of pregnancy care, usually performed between 20 – 22 weeks. It provides a detailed look at your baby’s development, checking everything from major organs to limb growth and placenta health. The morphology scan will also look at your cervix.
Many parents have questions about what to expect, including how accurate the scan is, whether it can detect all abnormalities, and if it will reveal the baby’s gender.
You might also wonder what happens if the baby is in a difficult position, whether you can bring a support person, or if additional scans might be needed.
In this fact sheet, we’ll answer these common questions so you can feel prepared and confident for your upcoming scan:
During a morphology scan, you’ll lie on an examination bed while the sonographer applies a warm ultrasound gel to your abdomen. This helps the ultrasound probe move smoothly and capture clear images. The scan is painless, though you may feel some light pressure as the sonographer moves the probe around to check different areas.
The sonographer will carefully examine your baby’s major organs, limbs, spine, brain, and face. They will also check the cervix, placenta, umbilical cord, and amniotic fluid levels to ensure everything is developing as expected. If the baby is in a difficult position, you may be asked to shift positions or take a short walk to encourage movement.
The scan usually takes 45 minutes, but this can vary depending on a variety of reasons such as fetal position or if there were any concerns visualised during the scan. If clear images aren’t obtained, you may need a follow-up scan. While the sonographer can explain what they’re looking at, the final report is sent to your doctor.
Fetal heart assessment
Can a Morphology Scan Detect Everything?
A morphology scan provides a detailed assessment of your baby’s development, but it can’t detect everything. It is primarily used to check for structural abnormalities in major organs, limbs, and the spine. However, some conditions may not be visible at this stage, and certain issues, such as genetic disorders, cannot be diagnosed through ultrasound alone.
If the scan raises any concerns or if the images are unclear, your doctor may recommend follow-up scans or additional tests. This could include another ultrasound at a later stage, a fetal echocardiogram to check the baby’s heart, or more advanced testing like amniocentesis or NIPT (non-invasive prenatal testing) if a genetic condition is suspected.
Results from the scan are performed from highly trained sonographers interpreted by specialist doctors (Obstetric and gynaecology sonologists or Maternal Fetal Medicine specialists).
Will My Morphology Scan Show My Baby’s Gender?
A morphology scan can usually detect your baby’s gender, but it’s not guaranteed. The sonographer determines gender by looking at the baby’s external genitalia on the ultrasound. If the baby is in a good position with clear visibility, gender identification is usually accurate.
However, several factors can affect how well the sonographer can see the baby’s anatomy. Baby’s position, gestational age, amniotic fluid levels, and maternal body composition can all impact clarity. While accuracy is generally high,gender predictions are not 100% certain, due to a variety of reasons.
If the sonographer can’t determine gender, they may suggest waiting until a later scan, such as a growth scan, where gender may be more visible or request that it be checked by the reporting QUFW doctor. Some parents also choose to confirm through non-invasive prenatal testing (NIPT). NIPT has a high detection rate for chromosomal abnormalities such as Trisomy 21. As the sex chromosomes are also assessed, gender may also be provided. As this is still only a screening test, correlation of the external genitalia by the ultrasound and the NIPT results is recommended.
Please note, you can choose to wait until birth to discover your baby’s gender! At QUFW, we will not tell you unless you ask or we have checked with you previously.
How Accurate Is a Morphology Scan?
A morphology scan is a highly detailed ultrasound, but it isn’t 100% accurate in detecting all abnormalities. While it provides a thorough check of your baby’s organs, limbs, and overall development, some conditions may not be visible due to the limitations of ultrasound technology.
Several factors can affect the clarity of images, including baby’s position, placenta location, amniotic fluid levels, and larger bodied person. If the baby is facing away or in a difficult position, some areas may be harder to assess, and a follow-up scan may be needed.
Certain conditions only become apparent later in pregnancy as the baby grows. Some heart defects, skeletal conditions, and developmental concerns may not be obvious at 20–22 weeks but could be detected in later scans. If needed, your doctor may recommend additional ultrasounds or further testing to monitor your baby’s health as your pregnancy progresses.
The Difference Between a Morphology Scan and Other Pregnancy Scans
A morphology scan is different from other pregnancy scans because it provides a detailed structural assessment of your baby’s development. Unlike a dating scan, which is done earlier in pregnancy to estimate your due date, the morphology scan checks major organs, limbs, and the placenta to ensure everything is forming as expected. A morphology scan also assesses your cervix.
A growth scan, on the other hand, is typically done later in pregnancy to monitor fetal size, amniotic fluid levels, and placental function, rather than looking for structural abnormalities.
The morphology scan is an important milestone because it can help identify potential abnormalities and provide reassurance that your baby is developing well. It also helps assess the placenta’s position, which is important for planning a safe delivery.
Sometimes, additional scans are needed. If the morphology scan is inconclusive, a follow-up ultrasound may be recommended. Other reasons for extra scans include concerns about baby’s growth, placenta function, or specific medical conditions.
You are welcome to bring up to two support people to your morphology scan at QUFW, and one of them may be a child. Having a partner, family member, or close friend with you can make the experience more special and provide emotional support.
However, since this is a medical procedure, it’s important that the sonographer can concentrate on capturing accurate images and measurements.
Also, if bringing a child, the second support person should be an adult who can supervise them, as ultrasounds can take time and may not always hold a child’s attention.
If your partner or family member can’t attend, you may consider video calling them briefly during the scan (please ask us beforehand) or sharing images afterward. If you are a surrogate patient, QUFW is happy to discuss your specific needs when booking your appointment.
What If My Baby Is Not in a Good Position for the Scan?
If your baby is not in an ideal position during the morphology scan, the sonographer will try different techniques to improve visibility. They may ask you to change positions, such as rolling onto your side, or they might gently press on your abdomen to encourage movement. Sometimes, a short break, walking around, or drinking cold water can help stimulate the baby to move into a better position.
If the sonographer still can’t get clear images, they may ask you to return for a repeat scan on another day. This is common and doesn’t necessarily mean something is wrong—just that the baby wasn’t positioned well enough for a full assessment. Your healthcare provider will let you know if a follow-up scan is needed and what to expect.
A morphology scan is a detailed ultrasound performed between 20 and 22 weeks of pregnancy to assess your baby’s development. It checks major organs, the spine, limbs, and facial features, as well as the placenta, amniotic fluid,umbilical cord, and cervix. Many parents wonder what to expect during the scan, how long it takes, and how to prepare.
In this fact sheet, we’ll walk you through the entire process, including how the scan is performed, what the sonographer looks for, and what happens if your baby is in a tricky position. Understanding these details can help you feel more prepared and confident for your appointment.
When you arrive for your morphology scan, you’ll check in at the clinic and may be asked to fill out some paperwork. A QUFW sonographer, who is specifically trained in pregnancy ultrasounds, will call you into the scan room and explain the procedure.
You’ll be asked to lie on an examination bed, and the sonographer will apply a warm ultrasound gel to your abdomen. This gel helps the ultrasound probe (transducer) glide smoothly over your skin and allows the ultrasound image to be created. The sonographer will then move the probe across your belly in different directions, capturing detailed images of your baby from multiple angles. They may need to apply gentle pressure to get a clearer view, particularly when examining specific organs or structures. If you have any concerns, please don’t hesitate to discuss this with your sonographer during your scan.
For more information about this process, read here.
What The Sonographer Looks For
During the morphology scan, the sonographer conducts a detailed examination of your baby’s development, carefully assessing key structures to ensure everything is forming as expected.
The scan focuses on major organs, including the brain, heart, kidneys, stomach, bladder, and liver. The sonographer checks for proper size, shape, and function, ensuring these vital organs are developing normally. The spine and limbs are also closely examined, with measurements taken to assess growth and symmetry. The face and skull are reviewed to check for any structural concerns, such as cleft lip or abnormalities in skull formation.
Beyond the baby, the scan also assesses your cervix, placenta, amniotic fluid levels, and umbilical cord. The placenta’s position is checked to rule out placenta previa, a condition where the placenta covers the cervix. Amniotic fluid levels are measured to ensure they are within a healthy range, as too much or too little fluid can indicate complications. The umbilical cord is examined for its structure and blood flow, as this is essential for delivering oxygen and nutrients to the baby.
Throughout the scan, the sonographer looks for markers of potential abnormalities. These are subtle indicators that might suggest certain conditions, such as chromosomal differences or structural concerns.
If any findings need further evaluation, your healthcare provider may recommend a follow-up scan or additional testing to gather more information. However, in most cases, the scan provides reassurance that your baby is growing and developing as expected.
Whether A Full Bladder Is Needed And How To Prepare
For most morphology scans, a moderately full bladder is required. A moderately full bladder can help lift the uterus and improve visibility, especially in earlier weeks.
To prepare, it’s best to wear loose, comfortable clothing that allows easy access to your abdomen. Some parents find that having a light meal or a cold drink before the scan may encourage the baby to move, which can help with imaging. If you’re unsure about any preparation requirements, check with us ahead of time.
How Long It Takes and What Results You Can Expect
A morphology scan typically takes 45 minutes, but this can vary depending on several factors. If the baby is in a good position, allowing the sonographer to capture all the necessary images easily, the scan may be completed more quickly. However, if the baby is facing away, curled up, or in a position that makes it difficult to assess certain structures, the scan may take longer or require a break to encourage movement.
If the baby’s position prevents a clear view of important areas, the sonographer may ask you to roll onto your side, adjust the tilt of the bed, stand up, or take a short walk to encourage movement. If the baby remains in a difficult position and the sonographer is unable to complete all necessary checks, you may need to return for a repeat scan on another day. This is common and doesn’t necessarily mean anything is wrong—it just ensures a thorough and accurate assessment.
In most cases, the sonographer will not provide detailed results immediately. Instead, they will complete the scan, document their findings, and discuss the information with a reporting QUFW doctor. If there are any concerns or unclear findings, the QUFW doctor may recommend further scans or tests for more information. If everything looks normal, no further action is needed, and the scan simply provides reassurance that your baby is developing well.
An Interview With Our Chief Sonographer, Teresa Clapham
We sat down with Teresa Clapham, Chief Sonographer at Queensland Ultrasound for Women (QUFW), to discuss the clinical importance of the morphology scan and what patients can expect from the experience.
A Comprehensive Assessment at Mid-Pregnancy
The morphology scan, also known as the 20-22 week scan, is a detailed structural assessment of the developing fetus. According to Teresa, its role extends far beyond simply checking the baby’s size or confirming gestational age.
“The morphology scan is our opportunity to assess all the baby’s major organ systems,” Teresa explains. “We look at the brain, spine, heart, kidneys, limbs, and facial structures. It’s a comprehensive screening tool designed to identify any structural anomalies that may affect pregnancy management or outcomes.”
While the scan is performed between 20 and 22 weeks, Teresa notes that the timing is carefully chosen to allow for optimal visibility of fetal anatomy while still offering time for appropriate follow-up if needed.
“By this stage, the baby is developed enough for us to visualise key structures, but we still have the option for further testing, referrals, or decisions if something unexpected is found,” she says.
More Than Just a Gender Reveal
For many parents, a common question is whether they’ll learn the baby’s sex during the scan. Many patients are already aware of the gender of their baby from their NIPT results. During the morphology examination the external genitalia is observed and correlated with the NIPT findings.
What the Scan Can, and Can’t, Detect
Despite the depth of the examination, not all conditions can be detected at the morphology scan. Teresa is clear about its limitations.
“Ultrasound has very good resolution, but there are conditions that may not be visible until later in pregnancy, or at all,” she explains. “Some anomalies are very subtle or may develop later. We always work within the boundaries of what imaging can show at a given stage.”
Patients are informed about the potential for incomplete visualisation, especially if factors such as maternal body habitus or fetal position make parts of the scan difficult.
“If we can’t see something clearly, we’ll recommend a follow-up scan. Our priority is to get accurate, complete information, even if that takes more than one appointment.”
A Shared Experience with Clinical Purpose
Many patients are surprised by how long the scan takes (often 30 to 45 minutes) and how still they’re required to remain.
“It’s a very focused process,” Teresa notes. “We capture and assess a multitudeof specific measurements and images. Some of that is diagnostic, but it’s also about record-keeping, making sure everything is documented clearly for the obstetric team.”
Support people are welcome at most morphology scans, and Teresa says it can be a powerful experience for families.
“It’s often the first time they’ve seen their baby in such detail. The heartbeat, the movement, even facial features, it’s emotional, and we don’t take that for granted.”
Still, she maintains that the role of the sonographer is firmly clinical.
“We love when parents are engaged and ask questions. Communication during the examination is integral in providing both a positive experience for the parents, but our first responsibility is also to do a thorough, systematic scan. That means there will be moments where we’re quiet and concentrating. That’s not a sign something’s wrong, it’s just how we work.”
Question: What does the sonographer do during a morphology scan?
During a morphology scan, the sonographer performs a detailed ultrasound assessment of the fetus, placenta, cervix, uterus, and amniotic fluid. The primary focus is to evaluate the baby’s anatomy and development, checking that major organs and structures are forming as expected. This includes examining the brain, face, spine, heart, lungs, stomach, kidneys, bladder, limbs, and umbilical cord. The sonographer also takes a series of biometric measurements (such as Biparietal diameter, head circumference, abdominal circumference, and femur length) to assess fetal growth and confirm gestational age.
The sonographer records a complete set of images for the obstetric team and may use colour Doppler to assess blood flow in certain areas, such as the heart or umbilical cord. If needed, they may ask you to change position or take a short break to encourage fetal movement and improve visibility.
Question: Can a morphology scan pick up all abnormalities?
No, a morphology scan cannot detect all abnormalities. While it is a highly detailed and systematic assessment, there are limitations to what can be seen on ultrasound, even when conditions are ideal. Some structural abnormalities are not visible until later in pregnancy, may develop after the scan, or may be too subtle to detect at this stage. Certain conditions, such as genetic or metabolic disorders, may not present with any visible features on ultrasound at all.
Detection also depends on factors such as fetal position, maternal body habitus, the presence of uterine fibroids or scarring, and the quality of ultrasound equipment. If an abnormality is suspected or if visibility is limited, the sonographer may recommend a follow-up scan, referral to a maternal–fetal medicine specialist, or further testing such as non-invasive prenatal testing (NIPT), amniocentesis, or MRI.
Question: Will the scan reveal my baby’s sex?
In most cases, yes. The morphology scan can reveal the baby’s sex if the baby is in a favourable position and visibility is clear. The sonographer will examine the external genitalia as part of the scan and can usually determine the sex with reasonable accuracy from around 16 weeks onward.
The sonographer’s main focus is on assessing fetal anatomy and development. If determining the sex is important to you, it’s best to let the sonographer know at the beginning of the appointment. In some cases, the baby’s position or movement may make it difficult to confirm with confidence. This is often correlated with prior NIPT results.
Question: How is a morphology scan different from other prenatal ultrasounds?
The morphology scan differs from other prenatal ultrasounds in its level of detail and its clinical purpose. While earlier scans (such as the dating scan or early anatomy/first trimester screening) focus on confirming pregnancy viability, estimating due date, and assessing early risk factors, the morphology scan provides a full structural review of the fetus at the mid-point of pregnancy (usually between 20 and 22 weeks).
Key differences include:
Scope of assessment: The morphology scan systematically examines each major organ system, measures fetal growth parameters, and evaluates the placenta, cord, uterus, and amniotic fluid. Earlier scans are more limited in what can be visualised due to the fetus’s smaller size.
Timing: Most general ultrasounds occur earlier (around 6–13 weeks) or later (after 28 weeks) and have different goals, such as confirming location, detecting multiple pregnancies, or monitoring growth and wellbeing. The morphology scan is timed specifically for optimal anatomical assessment.
Duration and complexity: The morphology scan usually takes longer and requires more precision. It may involve colour Doppler or additional imaging techniques to assess cardiac and vascular structures. The findings are used to inform pregnancy care and, if necessary, plan for further investigations or specialist referral.
Question: Am I allowed to bring a support person to the scan appointment?
You’re welcome to bring up to two support people to your morphology scan at QUFW. One of these may be a child, provided they are accompanied by an adult who can supervise them during the appointment. Ultrasound scans can take time and involve extended periods of stillness, so it’s important that children are occupied and cared for throughout.
Having a partner, relative, or close friend with you can offer reassurance and make the experience more meaningful. However, as this is a clinical assessment, your sonographer will need to remain focused to ensure precise imaging and measurements.
If your support person can’t be present, you’re welcome to briefly video call them during the scan, where appropriate. Please speak with our staff beforehand to check suitability. For patients attending as surrogates, our team can accommodate specific arrangements and will be happy to discuss this when you book.
Question: What happens if the baby isn’t in the right position to be scanned clearly?
If the baby is not in an ideal position during the scan, the sonographer may ask you to change positions, go for a short walk, or return later in the day. These strategies can encourage the baby to move into a better position, making it easier to obtain clear views of the necessary structures.
In some cases, not all areas can be adequately assessed during the appointment. If this occurs, you may be asked to return for a follow-up scan to complete the assessment. This is relatively common and does not necessarily mean there is a problem, it simply ensures the sonographer can obtain the full set of diagnostic images required for accurate reporting.
Question: What structural anomalies are most commonly assessed during a morphology scan?
During a morphology scan, the sonographer systematically examines the fetus for a range of structural anomalies. These assessments focus on identifying abnormalities that could affect health, development, or require further investigation during pregnancy or after birth.
Commonly assessed areas include:
Central nervous system: Assessment of the brain structures (ventricles, cerebellum, midline) and spine to check for neural tube defects such as spina bifida.
Cardiac structures: Visualisation of the four chambers of the heart, outflow tracts, and great vessels to detect congenital heart defects such as ventricular septal defects or transposition of the great arteries.
Face and neck: Checking for cleft lip or palate, abnormal facial profile, or neck masses.
Abdominal wall and organs: Evaluation of the abdominal wall (for defects such as gastroschisis or omphalocele), stomach, kidneys, bladder, and bowel.
Skeletal system: Assessing limb presence, length, and symmetry to identify limb reduction defects or skeletal dysplasias.
Thorax and lungs: Ensuring normal chest shape and size and identifying masses or signs of diaphragmatic hernia.
Each area is reviewed with multiple cross-sectional images to look for structural deviations. If an abnormality is detected, the patient may be referred for further follow up ultrasound scans (such as a fetal echocardiogram), a fetal MRI depending on the abnormality or further genetic counselling, depending on the findings.
Question: How is foetal biometry used to assess gestational age and growth at the 20–22 week scan?
Fetal biometry involves taking standardised measurements of the fetus to assess both gestational age and growth patterns. At the 20–22 week morphology scan, these measurements help confirm whether the baby is growing in line with expected milestones for the given stage of pregnancy.
Key biometric parameters include:
Biparietal diameter (BPD) – measures the width of the skull at the level of the thalami.
Head circumference (HC) – provides a more comprehensive assessment of head size and development.
Abdominal circumference (AC) – reflects fetal growth and is sensitive to growth restriction or macrosomia.
Femur length (FL) – measures the length of the thigh bone, contributing to overall growth assessment.
These values are compared against gestational age norms to evaluate whether growth is within expected ranges. If measurements fall significantly outside normal parameters, it may prompt further monitoring or investigation to rule out conditions such as intrauterine growth restriction (IUGR), macrosomia, or skeletal dysplasia. Biometry also supports the confirmation of due dates established earlier in pregnancy, though dating is most accurate in the first trimester.
Question: What follow-up investigations are recommended if a soft marker or structural anomaly is detected?
If a structural anomaly is detected during the morphology scan, the next steps depend on the nature, number, and severity of the findings, as well as the patient’s risk factors and preferences. Our QUFW maternal fetal medicine (MFM) and COGU Sonologists will discuss the findings and provide you and your doctor with any further follow up recommendations. Common follow-up investigations include:
Referral for further imaging: Further follow up ultrasounds within QUFW, fetal echocardiography at a Tertiary clinic may be organised to provide further clarity or information.
Non-invasive prenatal testing (NIPT): A blood test that analyses fetal DNA circulating in maternal blood to screen for common chromosomal abnormalities such as trisomy 21, 18, and 13.
Amniocentesis: A diagnostic test that samples amniotic fluid to directly analyse the fetal chromosomes or genetic material. This is usually offered when there is a significant concern about a genetic condition.
Fetal MRI: Occasionally used if a central nervous system abnormality is suspected and further anatomical detail is needed beyond what ultrasound can provide.
Serial growth scans: If the anomaly relates to growth parameters or placental function, repeat ultrasounds may be scheduled to monitor fetal growth and wellbeing over time.
Genetic counselling: Offered to help parents understand the potential implications of findings, the likelihood of recurrence, and available testing or support options.
Each case is reviewed individually, and the care team works with the patient to determine the most appropriate pathway based on clinical evidence and personal values.
Book Your Morphology Scan With QUFW
Queensland Ultrasound for Women (QUFW) offers comprehensive morphology scans at four convenient locations across South East Queensland. Our sonographers use advanced imaging technology to provide detailed assessments in a professional, supportive environment.