
Endometriosis is a complex and often misunderstood condition that can have a significant impact on quality of life. Many patients live with symptoms for years before receiving clear answers, and it is common to feel uncertain or frustrated during the diagnostic process.
This fact sheet explains what an endometriosis ultrasound assessment involves, why it is performed, and how it fits into diagnosis and treatment planning. In this article, Jacqui, Lead Gynaecological Sonographer at QUFW, talks you through what to expect from your assessment, the different types of endometriosis, and why specialised imaging plays such an important role.
Medical disclaimer: The information in this article is general in nature and provided for educational purposes only. It does not replace medical advice, diagnosis, or treatment. Please consult your doctor or specialist for personalised care.
Table of contents
- What is endometriosis?
- What are the symptoms of endometriosis?
- Why is endometriosis diagnosis often delayed?
- What are the different types of endometriosis?
- What is adenomyosis and its relationship to endometriosis?
- How is an endometriosis ultrasound performed?
- What will I feel during and after an endometriosis scan?
- Ultrasound, MRI, and laparoscopy: how they compare
- Book your gynaecology scan at QUFW
- References
- Video transcript
What is endometriosis?
Endometriosis is a condition where tissue similar to the lining of the uterus grows outside the uterus. These implants can attach to the ovaries, fallopian tubes, bowel, bladder, and other pelvic or abdominal structures.
“Endometriosis is a condition where tissue similar to the lining of the uterus grows outside the uterus,” Jacqui explains in the above video.
Like the uterine lining, this tissue responds to hormonal changes during the menstrual cycle.
“Just as the lining of the uterus thickens and bleeds every month during menstruation, so does this tissue.”
Because the blood and inflammatory fluid cannot drain away normally, this process leads to inflammation, swelling, scarring, and pain.

Ultrasound image of an endometrioma in the left ovary
What are the symptoms of endometriosis?
Endometriosis affects up to one in seven women.
Symptoms vary widely.
“Some people have no pain at all, while others have debilitating symptoms,” says Jacqui.
Common symptoms include:
- Painful periods
- Chronic pelvic pain
- Pain during or after sexual intercourse
- Painful bowel motions during menstruation
- Abnormal bleeding
- Pain with urination
- Pain with ovulation
- Fatigue
About 30% of patients with endometriosis experience infertility, and symptoms do not always correlate with disease severity.
Why is endometriosis diagnosis often delayed?
In Australia, the average diagnostic delay for endometriosis is approximately 6.4 years.
“Period pain is often dismissed as normal,” Jacqui explains.
Other contributing factors include:
- Misdiagnosis at GP or imaging level
- Limited access to specialised imaging
- Long public hospital surgical waitlists
- A shortage of surgeons trained in deep endometriosis surgery
What are the different types of endometriosis?
There are three recognised types of endometriosis, each with different imaging features and clinical implications.
Endometriomas
Endometriomas, often called chocolate cysts, are cysts that form on the ovaries.
“They occur in around 17 to 44% of patients with endometriosis,” Jacqui explains.
They are usually visible on transvaginal ultrasound and act as a warning sign that further assessment of the pelvis is needed.
Superficial endometriosis
Superficial endometriosis accounts for around 80% of cases and involves small lesions on the peritoneal surface.
“Superficial endometriosis is the most subtle form of the disease,” says Jacqui.
Although difficult to detect, advancements in ultrasound technology now enable our team to sometimes directly visualise superficial endometriosis. This is a huge leap forward in the diagnosis of the condition.
Also, while a negative transvaginal scan doesn’t reliably confirm the absence of the disease, a positive transvaginal scan for superficial endometriosis may facilitate a non-invasive diagnosis which may ensure early treatment, prevent progression, and improve outcomes.
“Some women with superficial endometriosis may have more severe symptoms than those with deep endometriosis, Jacqui says”
Deep endometriosis
Deep endometriosis is now considered to be any invasion beyond the peritoneal surface.
“It causes scarring and adhesions that can distort normal anatomy,” Jacqui explains.
It affects 15 to 30% of patients and commonly involves:
- Uterosacral ligaments
- Posterior vaginal wall
- Bowel
- Bladder
It is important to understand the difference between superficial endometriosis and deep endometriosis. The latest consensus is that superficial endometriosis should be characterised as a disease that lines the surface of the peritoneum. Any invasion beyond the peritoneal surface is considered deep endometriosis.
What is adenomyosis and its relationship to endometriosis?
Adenomyosis is a separate but related condition where endometrial tissue grows into the muscle wall of the uterus.
“It is commonly diagnosed in women between 40 and 60, however it has been confirmed in younger women,” says Jacqui.
Symptoms often include heavy and painful periods, and adenomyosis frequently coexists with endometriosis.
How is an endometriosis ultrasound performed?
Your assessment begins with a detailed gynaecological history.
First, a transabdominal ultrasound is performed with a full bladder to assess the pelvis and kidneys. This scan provides an overview but does not show deep endometriosis in detail.
“The main endometriosis assessment is performed transvaginally,” Jacqui explains.
The internal scan uses a slender probe with a sterile cover. With your consent, it is gently inserted after you empty your bladder.
During the scan:
- The probe is angled carefully to assess pelvic structures
- Gentle pressure may be applied to assess organ mobility
- The uterus, ovaries, bowel, bladder, and ligaments are examined
“The entire ultrasound assessment takes about 30 minutes and follows well-established protocols.”
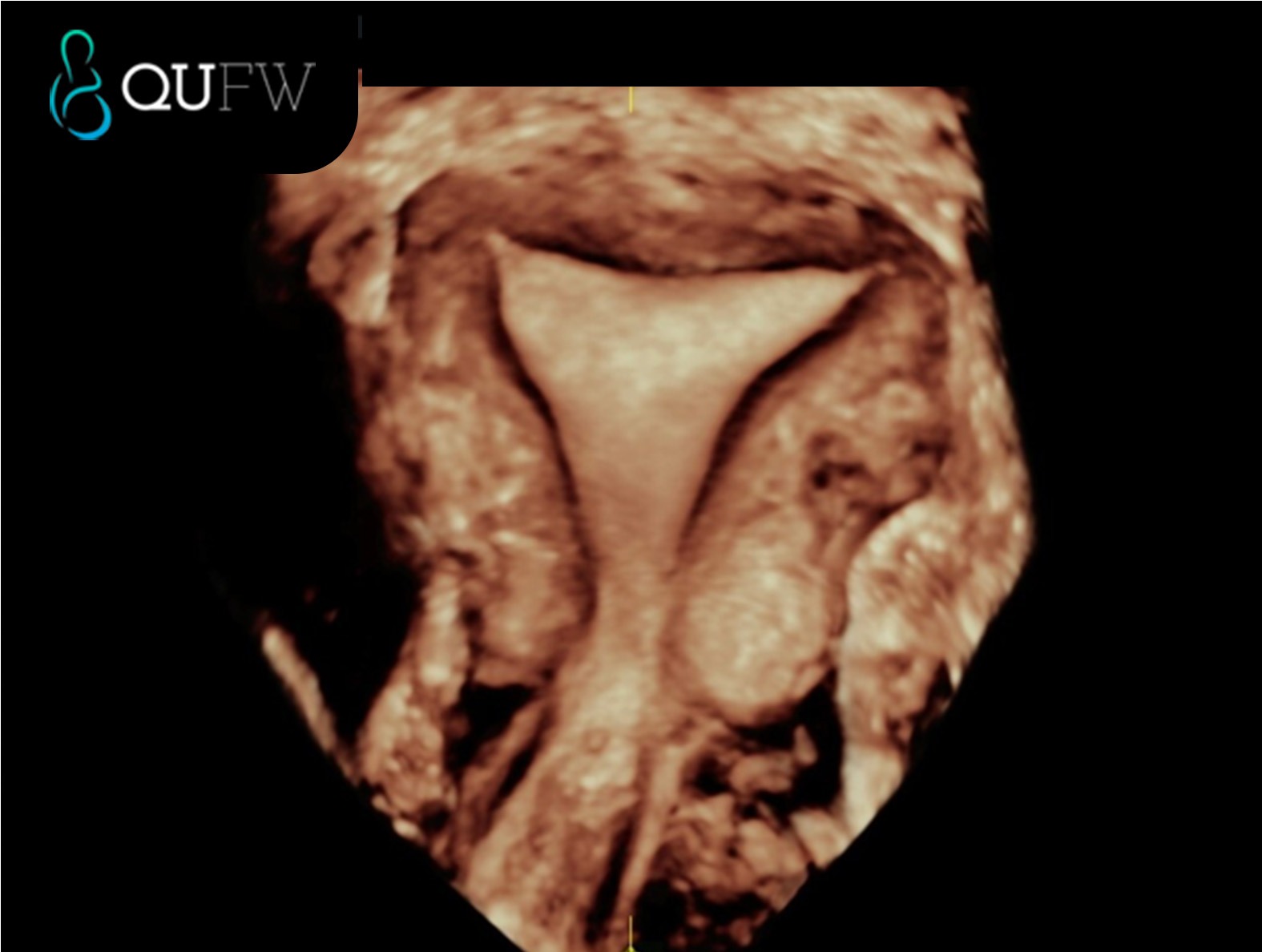
3D reconstructed coronal image of the uterus
What will I feel during and after an endometriosis scan?
Some patients experience tenderness during the examination, particularly if endometriosis is present.
“Some women may not be able to tolerate a transvaginal scan due to intense pain,” Jacqui notes.
Options to support comfort include:
- Pain relief before the appointment
- Pelvic floor physiotherapy for relaxation techniques
After the scan, mild pain or spotting can occur and usually settles quickly.
“It’s also common to feel emotional after receiving an endometriosis diagnosis,” Jacqui explains.
Ultrasound, MRI, and laparoscopy: how they compare
MRI can be used when a transvaginal scan is not tolerated, but it has limitations.
“MRI is not a dynamic study and cannot assess whether the pelvic organs are stuck together,” Jacqui explains.
Laparoscopy remains a treatment tool but is no longer required purely for diagnosis when high-quality ultrasound is available.
Book your gynaecology scan at QUFW
Living with suspected endometriosis can feel isolating, especially when answers have taken years to find. Many patients describe relief when their pain is finally taken seriously, even if the path forward still feels uncertain.
At QUFW, gynaecology scans are designed to provide clarity, validation, and accurate information to support your care. Your assessment is performed using specialised protocols and interpreted by clinicians with advanced expertise in gynaecological ultrasound and endometriosis. Contact us here.
The goal is to give you and your healthcare team the information needed to make informed decisions about next steps, whether that involves ongoing monitoring, medical management, or surgical planning.
We are here for you.
References
- Guerriero, S., Condous, G., van den Bosch, T. et al. (2016). Systematic approach to sonographic evaluation of the pelvis in women with suspected endometriosis. Ultrasound in Obstetrics & Gynaecology, 48(3), 318–332. https://obgyn.onlinelibrary.wiley.com/doi/10.1002/uog.15955
- Nisenblat, V., Bossuyt, P. M., Shaikh, R. et al. (2016). Blood biomarkers for the non-invasive diagnosis of endometriosis. Cochrane Database of Systematic Reviews, Issue 5. https://pubmed.ncbi.nlm.nih.gov/27132058/
Transcript
Hi, my name’s Jacqui. I’m the lead gynaecological sonographer for QUFW, and I’m here to talk you through your endometriosis assessment.
Endometriosis is a condition where tissue similar to the lining of the uterus grows outside the uterus. It commonly attaches to the ovaries, fallopian tubes, bowel, and bladder, as well as other organs. Just as the lining of the uterus thickens and bleeds every month during menstruation, so does this tissue. This causes inflammation, swelling, and pain in these areas.
Endometriosis affects as many as one in seven women and people assigned female at birth. Some people have no pain at all, while others have debilitating symptoms such as pain during periods, chronic pelvic pain, pain with sexual intercourse, painful bowel motions during menstruation, abnormal bleeding, pain with urination, pain with ovulation, and fatigue. About 30% of patients with endometriosis experience infertility. In Australia, the average person with endometriosis experiences a diagnostic delay of about 6.4 years.
Why is there a delay in diagnosis?
Period pain is often dismissed as normal. There is also frequent misdiagnosis at the GP level, during imaging, or even at laparoscopy. Public hospital waitlists for surgery can be long, and there are not enough trained surgeons to perform specialised deep endometriosis surgery. There are also limited numbers of trained sonographers to perform advanced endometriosis ultrasounds, and not enough specialists able to accurately report these assessments.
There are three types of endometriosis. The first type is endometriomas, the second is superficial endometriosis, and the third is deep endometriosis.
Endometriomas, also known as chocolate cysts, occur in around 17 to 44% of patients with endometriosis. They can vary in size and may appear on one or both ovaries. They are a warning sign that calls for a thorough investigation of the entire pelvis and are usually easy to see on transvaginal ultrasound.
Superficial endometriosis is the most subtle form of the disease and accounts for about 80% of cases. Ultrasound can sometimes give indications of superficial endometriosis when there is tenderness in a particular area or when the organs appear stuck. In the past, ultrasound had limited sensitivity in detecting superficial endometriosis because the lesions are small and have little volume. However, with ongoing research, we are beginning to see both direct and indirect features of this type. Some women with superficial endometriosis may have more severe symptoms than those with deep endometriosis.
Deep endometriosis is defined as lesions that extend more than five millimetres beneath the peritoneum. It causes scarring and adhesions that can distort normal anatomy. Deep endometriosis accounts for 15 to 30% of cases and is often found on the posterior vaginal wall behind the cervix, the uterosacral ligaments, the bowel, and the bladder. It’s less frequently seen on the ureters, diaphragm, or in surgical scars.
Adenomyosis is another benign gynaecological condition, commonly diagnosed in women between the ages of 40 and 60. It occurs when endometrial tissue grows into the muscle wall of the uterus. Common symptoms include painful and heavy periods. Endometriosis and adenomyosis can often occur together.
How is the ultrasound performed?
First, your gynaecological history is taken. Then a transabdominal scan is performed while your bladder is full. This gives us an overview of your pelvis and allows us to assess your kidneys. The transabdominal scan will not provide detailed information about deep endometriosis.
The main endometriosis assessment is performed transvaginally, using an internal probe that functions like a slender camera. For your comfort and to optimise our views, you’ll be asked to empty your bladder before the internal scan. A sterile probe cover is used, and with your consent, the probe is gently inserted into the vagina.
During the examination, the probe is moved at different angles, and the sonographer may place a hand on your abdomen to apply light pressure and assess the mobility of your uterus and ovaries. The entire ultrasound assessment takes about 30 minutes and follows well-established protocols. The results are often discussed with you, and the report will be sent to your referring doctor in a timely manner.
If you have never had penetrative sexual intercourse or used tampons, a transvaginal scan is still possible with a skilled sonographer and your consent. Some patients experience tenderness, so options include taking pain relief before the appointment. Pelvic floor physiotherapists can also help with relaxation techniques.
Some women, however, may not be able to tolerate a transvaginal scan due to intense pain. In these cases, MRI can be used as an alternative. However, MRI is not a dynamic study and cannot assess whether the pelvic organs are stuck together due to adhesions from endometriosis.
After the transvaginal examination, some women can experience mild pain, which is considered normal. Occasionally, the examination may temporarily increase your pain, but this usually resolves after the ultrasound. Pain relief can be used to ease any discomfort. Some women may also experience light spotting.
It’s also common to feel emotional after receiving an endometriosis diagnosis. Some women feel relieved that their pain has been validated, while others may feel disappointed if the ultrasound appears normal. A normal ultrasound performed by a trained specialist does not rule out all endometriosis. Ultrasound has limitations in diagnosing superficial endometriosis, which is the most common type, affecting about 80% of patients.
The severity of the disease does not always match the severity of symptoms. Some women with superficial endometriosis have more severe pain than those with deep endometriosis. If symptoms cannot be managed, a laparoscopy may be necessary.
If you already have symptoms of endometriosis, do you still need an ultrasound before surgery?
Yes. The aim is to reduce unnecessary surgery, which can cause scarring, adhesions, and further damage to the pelvic organs. The presence of bowel or deep endometriosis suggests that an advanced laparoscopic surgeon should perform the operation rather than a general laparoscopic surgeon.
A transvaginal ultrasound has been shown to have higher sensitivity in detecting deep endometriosis compared to diagnostic laparoscopy. This non-invasive approach allows the disease to be mapped and may reduce the need for diagnostic surgery and surgical surprises.
If you’ve already had an ultrasound that confirms endometriosis, do you need surgery to confirm your diagnosis?
No. A transvaginal ultrasound is an accurate, non-invasive diagnostic tool. There’s no need to confirm the findings with a laparoscopy. If endometriosis is identified on your ultrasound, it gives you and your healthcare team more accurate information to plan your treatment. This may involve surgical removal of endometriosis or non-surgical management.
What is the difference between a standard pelvic ultrasound and a specialised endometriosis assessment?
A standard pelvic ultrasound assesses the uterus and ovaries. This routine scan can detect endometriomas but often misses deep endometriosis affecting structures outside the uterus.
A specialised endometriosis assessment goes beyond these areas to examine the bowel, bladder, and supporting ligaments in both the anterior and posterior compartments. If these areas are not assessed, deep endometriosis may not be detected.
A specialised endometriosis ultrasound is performed by trained specialists using dynamic techniques to assess for organ mobility and adhesions. This method can detect deep endometriosis with high accuracy and sometimes superficial disease as well.
At QUFW, your specialised endometriosis assessment is performed and reported by an expert-trained gynaecologist with advanced skills in interpreting all aspects of endometriosis on ultrasound.
We are here for you.
====================
Content Disclaimer
The information provided on this website is for educational and informational purposes only. It is not intended as a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your obstetric doctor or other qualified provider with any questions you may have regarding a medical condition or treatment and before undertaking a new healthcare regimen.
The content on this website is not intended to be a comprehensive source of information on any particular topic and should not be relied upon as such. The authors and publishers of this website are not liable for any damages or injury resulting from the use or misuse of the information provided on this website.
0 Comments