
In early pregnancy, you might hear a range of terms used for the scans you might need, such as “viability,” “dating,” “early anatomy,” or “NIPT.” These names can sound similar, and it’s not always clear how they differ or when each one is recommended.
This fact sheet explains the different types of early pregnancy scans so you can understand their purpose and timing. It answers the following questions:
- Overview of first-trimester scans
- Dating and Viability scan (around 6–12 weeks)
- Early Anatomy scan (13–13+6 weeks)
- First Trimester Combined Screening (FTCS) (13–13+6 weeks)
- NIPT and its timing
- Which scan should I book first?
—————
1. Overview of first-trimester scans
In the first trimester, ultrasound can confirm pregnancy, check wellbeing, and estimate due dates.
Common scans include:
- Viability and Dating scan – a viability scan or a dating scan refer to the same thing and involve an early check of pregnancy location and heartbeat. The Sonographer measures the fetus to establish or confirm an estimated due date (EDD)
- Early Anatomy scan – assesses early anatomy and screens for certain structural conditions
- First Trimester Combined Screening scan – this scan is the same as the Early anatomy scan but provides additional screening for chromosomal abnormalities, particularly Trisomy 21, 18 and 13. The risk assessment is only performed if the patient has not had a NIPT performed. The NIPT has a higher detection rate for Trisomy 21 (almost 99% detection rate) as opposed to approximately 90% detection rate.
- NIPT (non-invasive prenatal testing) – blood test for chromosomal screening, recommended to be accompanied alongside a viability ultrasound.
Here’s a breakdown of each of these scans:
2. Dating and Viability scan (around 6–12 weeks)
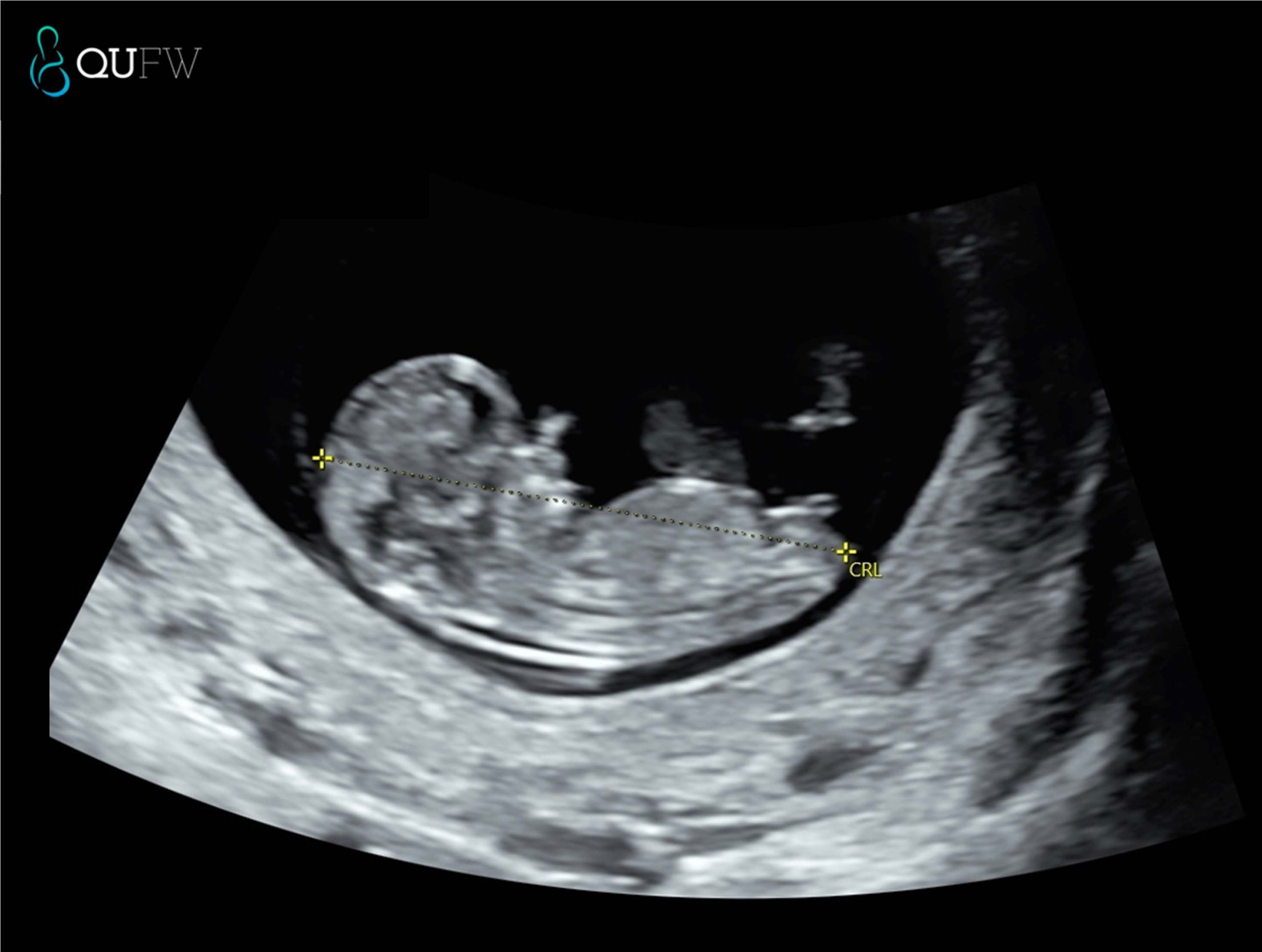
A viability scan confirms that the pregnancy is in the uterus, checks for a heartbeat, and assesses early development. A dating scan measures the crown–rump length (CRL) to estimate gestational age and your EDD. This timing offers a high degree of accuracy (± 5 days). You may be referred for a viability scan if you:
- Have pain or bleeding
- Have had an ectopic pregnancy before
- Conceived via IVF
- Have a history of pregnancy loss
It also confirms:
- The baby’s heartbeat
- Whether you are carrying one baby or multiples
- The pregnancy location
If performed very early (before 6 weeks), it may be too soon to see a heartbeat, and a repeat scan may be needed.
Dating scan prior to NIPT
3. Early Anatomy scan (13–13+6 weeks)
The Early Anatomy scan assesses early development and screens for specific structural anomalies. At QUFW we also perform a risk assessment for pre-eclampsia at this scan. The early anatomy scan is performed in conjunction with an NIPT. If you elect not to have NIPT then you will be asked if you would like a risk assessment for Trisomy 21, 18 and 13 (the most common chromosomal anomalies) performed in addition to the anatomical assessment, in which case this then becomes a FTCS (see below).
It also checks:
- Heartbeat
- Cervical length assessment
- Placenta position
- Multiple pregnancy details
4. If the scan’s EDD differs from your LMP-based date, your healthcare provider will usually use the ultrasound date.
This is the same as an early anatomy scan, however we provide a risk assessment for chromosomal abnormalities like Trisomy 21, 18, and 13. As a screening for Down Syndrome, it has approx. 90% detection rate when combining the following factors such as
- Maternal age and background risk
- Ultrasound markers such as nuchal translucency, nasal bone, fetal heart rate
- Maternal serum biochemistry (Free beta-hCG and PAPP-A)
At QUFW, similar to the Early Anatomy scan we also perform a pre-eclampsia risk assessment as part of this scan.

Nuchal translucency assessment
5. NIPT and its timing
NIPT is a blood test that can be done from around 10 weeks of pregnancy. At QUFW, we prefer to book NIPT’s from 10 weeks 2 days at the earliest.
It analyses small fragments of the baby’s DNA in the mother’s blood to assess the likelihood of certain chromosomal conditions. NIPT does not replace ultrasound which assesses for structural abnormalities.
6. Which scan should I book first?
It depends on your history and how certain you are of your dates:
- Uncertain LMP or irregular cycles – dating and viability scan between 7–12 weeks
- History of pregnancy complications – Viability and dating scan from 6 weeks gestation
- IVF conception – viability scan at 6–7 weeks, then Early Anatomy scan at 13–13+6 weeks
- Known LMP and no risk factors – dating and viability scan between 7-12 weeks, followed by an Early Anatomy scan. Your GP or specialist will recommend a plan suited to your circumstances.
FAQs
Is a viability scan the same as a dating scan?
A viability and dating scan is essentially the same scan and confirms the presence of a pregnancy in the correct location, if it is a multiple pregnancy and confirms that a heart beat is present. It is also used to either confirm or establish correct dating or due date for the pregnancy.
Do I need both Early Anatomy and NIPT?
A NIPT is a screening test for chromosomal abnormalities. It does not detect structural or developmental concerns with the developing fetus. It is advised that an Early Anatomy scan is performed between 13 – 13 weeks 6 days as a structural assessment of your baby. At QUFW we also perform a Preeclampsia screening as a component of the Early Anatomy scan. A low probability result for a NIPT, does not exclude a structural concern in a pregnancy.
When is the best time for a dating scan?
Between 7 and 12 weeks for best accuracy.
Can an Early Anatomy scan detect all conditions?
No. It screens for certain conditions but not all genetic or structural differences may be detected at this early gestation. A further morphology scan is recommended between 20-22 weeks to reassess the baby.
====================
Content Disclaimer
The information provided on this website is for educational and informational purposes only. It is not intended as a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your obstetric doctor or other qualified provider with any questions you may have regarding a medical condition or treatment and before undertaking a new healthcare regimen.
The content on this website is not intended to be a comprehensive source of information on any particular topic and should not be relied upon as such. The authors and publishers of this website are not liable for any damages or injury resulting from the use or misuse of the information provided on this website.
0 Comments